
Dr. Robert Miller treats a young patient with a durable esthetic restoration choice
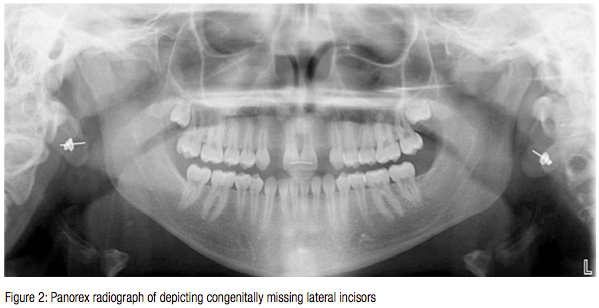
A 19-year-old female presented for the replacement of her congenitally missing lateral incisors (Figures 1 and 2). She had recently completed orthodontic therapy, which included interceptive orthodontics in the mixed dentition stage to create appropriate space for lateral incisors. We were comfortable with placing implants at this stage as “serial cephs” depicted that jaw development has been completed (Figure 3).
A CT scan was exposed to ensure adequate ridge dimension and proper root alignment for implant placement (Figures 4 and 5). Upon consultation with her restorative dentist, it was decided that the restoration of choice would be all ceramic with custom-milled zirconia abutments. We chose to use two Straumann® Narrow CrossFit® Roxolid® Bone Level fixtures (Figure 6). The bone level implant is designed to provide the restorative dentist with the most restorative options, including custom-milled ceramic abutment that averts metal collar exposure or the potential for a dark hue at the gingival margin in patients with a thin tissue biotype. The Roxolid implant with its increased tensile strength, when compared to titanium, enables the surgeon to place a smaller diameter fixture that maximizes the amount of native bone buccal and palatal (lingual) to the fixture body.1 The SLActive hydrophilic surface was designed to reduce time needed for osseointegration, thereby speeding up healing times and increasing the confidence of the clinicians.2,3
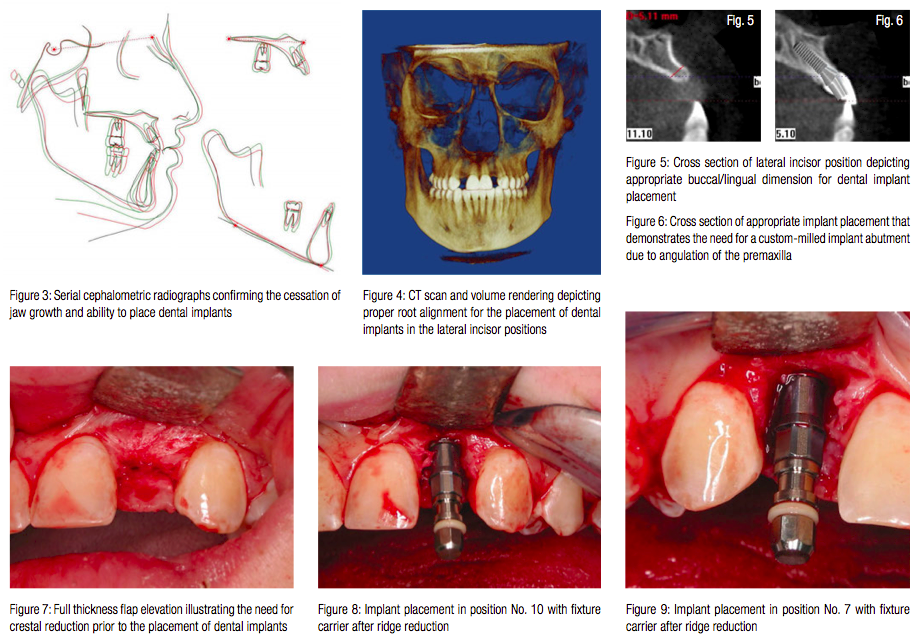
The CT scan depicted an issue with the level of the osseous crest with respect to the adjacent teeth. Appropriate three-dimensional placement for this patient necessitated the removal of 3–4 mm of (vertical) bone to accommodate the restorative abutment and allow for the development of the emergence profile of the restorations. This additional room gives the laboratory technician adequate space for an esthetic restoration with appropriate dimensions and contours.

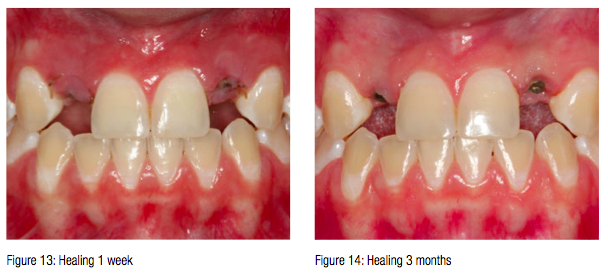
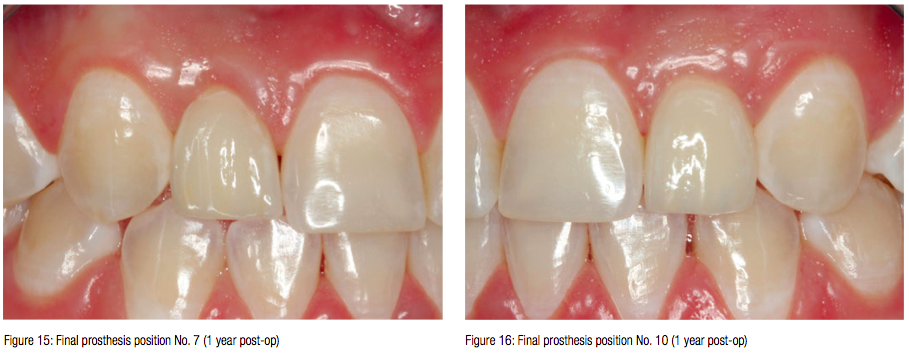
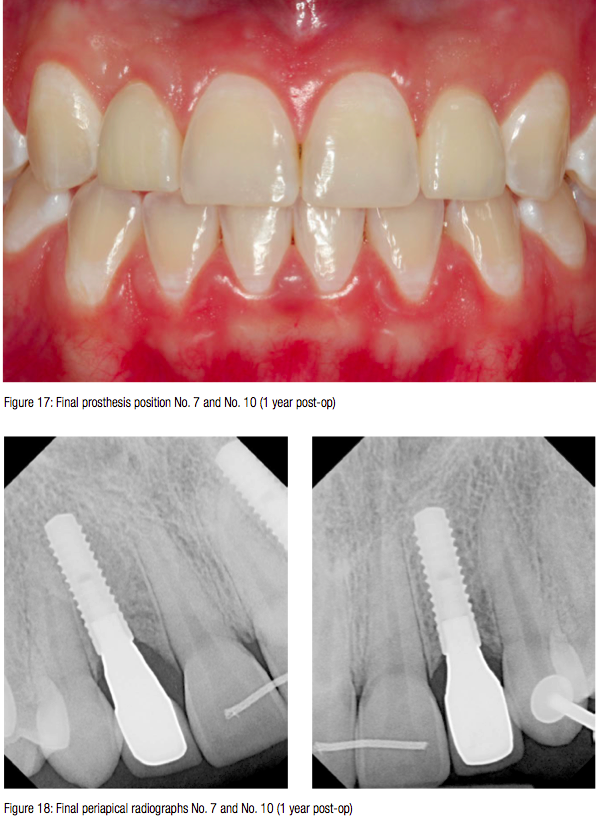
Full thickness buccal and palatal flap elevation was necessary to visualize the osseous crest (Figure 7). Reduction of the ridge was accomplished with a round diamond bur and high-speed hand piece. Optimal positioning of the fixtures is 3 mm apical to the adjacent cemento-enamel junctions (Figures 8 and 9). Two 3.3 mm x 12 mm Straumann Roxolid NC Bone Level implants were placed with Straumann 3.6 mm x 3.5 mm healing abutments (Figure 10). The Hawley orthodontic retainer was adjusted and used as a provisional during the osseointegration phase (Figures 11 and 12). Healing was uneventful and was referred for restoration after 3 months of hard and soft tissue maturation (Figures 13 and 14). As planned, the final restoration was an all ceramic restoration with a custom-milled zirconia abutment (Figures 15–18).
The patient was ecstatic with her restorations. Having congenitally missing teeth has plagued her throughout her life. She was extremely self-conscious having to wear a removable appliance which she believed inhibited her ability to develop relationships. Upon completion, she had renewed self-confidence and reports that she is now socially active and is pursuing a career in sales. She believes that this has been a life-altering event.
Placement of dental implants for young adults has an added responsibility because the fact that the implant has to last their lifetime, which according to statistics is greater than 65 years.
It is incumbent upon clinicians to choose a system that is based on sound clinical testing and will withstand the test of time. It is also important to choose a company that will be in business to stand by their products. The fabrication of anterior restorations that are indistinguishable from the existing teeth is one of the most difficult tasks that a dentist can undertake. Treatment planning from the restoration back includes having to choose the appropriate implant as well as the company. The Straumann Roxolid Bone Level implant fit the criteria that were necessary to ensure an esthetic restoration with the longevity necessary for this young adult.
Thank you to Dr. Peter Wohlgemuth for the orthodontic therapy and Dr. Arthur Stanger for the prosthetics.
- Data on file.
- From 6–8 weeks to 3–4 weeks compared to SLA®.
- Straumann SLActive® Scientific Overview (USLIT196).
Stay Relevant With Implant Practice US
Join our email list for CE courses and webinars, articles and mores
