Drs. Paras Ahmad, Jake Zellner, Michael A Pikos, Richard Miron, and Georgios A. Kotsakis delve into the intricacies of peri-implant maintenance.

Drs. Paras Ahmad, Jake Zellner, Michael A Pikos, Richard Miron, and Georgios A. Kotsakis discuss the importance of preserving titanium surface integrity
Mechanical implant surface cleaning remains a constituent of peri-implantitis therapy, but its standalone effectiveness is increasingly called into question in light of titanium particle-induced inflammation. The evolving comprehension of peri-implantitis as a condition shaped by both material and microbial-driven determinants highlights the requirement for biomaterial-aware and integrative therapeutic approaches that address both the physicochemical and biological intricacies of the condition.1
1. Preserving titanium integrity in peri-implant decontamination
Mechanical debridement remains a cornerstone of peri-implantitis therapy due to its ability to disrupt microbial biofilms.2 However, conventional approaches employing ultrasonic scalers with metal tips or titanium curettes have raised concerns regarding iatrogenic surface damage.3 In vitro and preclinical studies demonstrate that abrasive instrumentation can disrupt the titanium-oxide passivation layer, generating titanium microparticles and nanoparticles that provoke inflammatory tissue responses and osteolytic activity, even in the absence of bacteria.4,5 These findings emphasize that surface preservation is not only desirable but essential to maintain peri-implant tissue health. Thus, the latest evidence-based guidelines, including the AAP/AO consensus,6 shifted the paradigm towards non-abrasive decontamination methods that prioritize both preservation of surface integrity and microbial control. In-vitro reports have shown that surface-friendly decontamination procedures not only minimize titanium particle release but also cause significantly enhanced re-osseointegration potential compared to their abrasive counterparts.7 Particularly, approaches using non-metallic instruments or water-jet irrigation have exhibited superior results regarding the preservation of the implant’s biocompatible surface characteristics and facilitating cell attachment, proliferation, and differentiation on previously contaminated implant surfaces.7
A pivotal advancement in this area was reported by Daubert, et al.,8 who provided the first human data substantiating the deleterious effects of abrasive mechanical instrumentation on titanium release and clinical outcomes. The study showed that using abrasive tools, i.e., titanium curettes, to clean implants can lead to nearly 10 times more titanium particle release over time in humans than when using gentler, nonabrasive methods. This wasn’t just seen in lab tests; in real patients, it was linked to deeper peri-implant probing depths remaining unresolved after treatment. These findings suggest that titanium particles released during aggressive cleaning may play a role in damaging the tissues around implants and worsening peri-implant disease.8
These outcomes highlight a critical evolution in the comprehension of the peri-implantitis treatment landscape: therapeutic efficacy must now be assessed not merely by biofilm removal but also by the ability to maintain the chemical and structural stability of the implant surface. In summary, the implant-host-microbiome interface is a delicate balance affected by both iatrogenic and biological factors. Chemical or mechanical trauma to the titanium surface can propagate or exacerbate inflammatory pathways, independent of microbial presence, hence decreasing the overall efficacy of conventional antimicrobial strategies.
2. Tailoring peri-implantitis therapy to implant-specific factors
Beyond their direct pro-inflammatory effects, titanium particles also seem to indirectly mediate disease severity by impairing host immune surveillance and promoting dysbiosis within the peri-implant microbiome.9 This shift in microbial ecology improves biofilm pathogenicity and may contribute to the well-documented resistance of peri-implant biofilms to conventional antimicrobial strategies.10
Biofilms, structured microbial communities encased in an extracellular polymeric matrix, demonstrate increased resistance to both antibiotic therapy and host immune mechanisms.11 The affinity of bacterial biofilms for titanium surfaces, combined with the anatomical limitations of accessing the subgingival peri-implant space, render effective decontamination particularly challenging. These mechanical and biological barriers mandate treatment strategies that go beyond conventional periodontal approaches, which were originally developed for natural dentition.11
In addition to biofilm-associated factors, other implant-specific, non-plaque-related contributors have been identified. One important example is excess dental cement, especially resin-based materials, which have been shown to induce peri-implant inflammation and bone loss when inadvertently retained in the peri-implant sulcus. Wilson has reported a causal association between peri-implantitis and excess submucosal cement, highlighting the necessity for rigorous cementation procedures in implant-supported restorations.12
Collectively, these outcomes reinforce the need for implant-specific treatment workflows that diverge from conventional periodontal procedures applied to teeth. The biological differences between implant surfaces and natural teeth, such as the absence of periodontal ligament as well as submucosal calculus in implants and varying connective tissue attachment, demand a tailored clinical strategy. One such workflow, devised by the authors and grounded in current evidence on implant surface preservation, emphasizes non-abrasive decontamination approaches and the identification of modifiable implant-specific predisposing factors.13 This stepwise protocol, referred to as the “Impla-Safe” protocol, is designed to maintain peri-implant tissue health while minimizing iatrogenic damage to the titanium surface, hence preserving the potential for re-osseointegration and long-term implant success (Figure 1).
Step 1: Peri-implant probing — approach and instrumentation 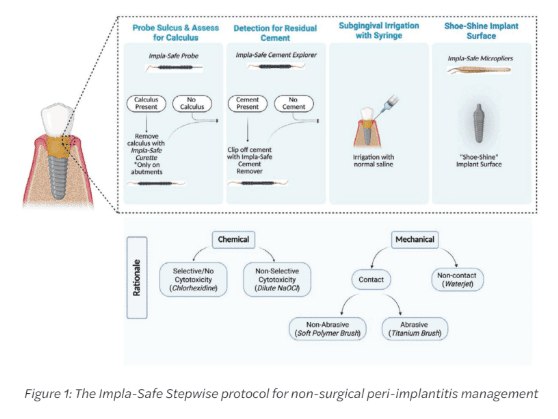
Accurate assessment of peri-implant tissue starts with adequate probing, which remains a critical step in the diagnosis of peri-implant diseases. Contrary to misconceptions, dental implants can and should be probed routinely to assess peri-implant mucosal health, such as bleeding on probing, PPD, and suppuration. Nonetheless, probing around implants needs modifications in technique owing to distinct histological and anatomical differences compared to natural teeth.
Unlike the robust connective tissue attachment around natural dentition, the peri-implant mucosa demonstrates a weaker epithelial attachment and lacks true connective tissue fiber insertion into the implant surface. This anatomical variation makes the peri-implant interface more prone to mechanical trauma during probing, requiring the use of decreased probing forces, generally not exceeding 0.25 N, to avoid disruption of the fragile soft tissue seal.
To facilitate accurate and gentle probing, the use of titanium implant-specific periodontal probes that have greater elasticity is recommended. Implant probes should be manufactured in a soft, and preferably titanium alloy, with a narrower and more elastic structure than conventional plastic or metal probes. Examples include the including the titanium Impla-Safe Probe (Salvin Dental, Charlotte, North Carolina) and the steel ACE probe (PDT, Missoula, Montana) that have flexible shafts with a very high elasticity modulus that improves tactile feedback by gently flexing upon contact with the implant surface, decreasing the risk of surface abrasion or iatrogenic trauma to the epithelium. This flexibility is important as a compensatory mechanism for the lack of elasticity of the peri-implant as compared to periodontal tissues. In essence, the lack of elasticity of the peri-implant tissues due to differences in collagen organization and attachment as compared to teeth is compensated for by the elasticity of the probe to prevent a tear in the peri-implant junctional seal that could be caused by the pressure exceeding the modulus of elasticity of the tissues. Moreover, unlike bulky plastic probes that may undermine accuracy and access, flexible probes permit a more precise evaluation of submucosal conditions while maintaining minimal invasiveness.
Step 1B: Management of calculus on dental implants — minimizing risk to titanium integrity
When calculus is detected during clinical evaluation of an implant site, careful attention must be paid to both its location and the biological implications of mechanical debridement. Published literature suggests that supramucosal calculus formation is relatively frequent on transmucosal abutments but rarely occurs on the submucosal “threaded” portions of the implant body. This discrepancy is mainly due to the structural and electrochemical variations between titanium oxide and natural tooth root cementum. Cementum, with its surface porosity and organic composition, enhances the retention and nucleation of mineralized deposits, while the more inert and smoother titanium oxide surface lacks these features, deeming submucosal calculus formation rare.
When a visible supramucosal calculus is found on prosthetic or abutment components, eradication should be conducted utilizing implant-safe nonabrasive instruments. Specifically, curettes made of soft titanium alloys, engineered to have a decreased Rockwell hardness (e.g., Wingrove Titanium curette, PDT, Missoula, Montana) than the implant fixture itself, are recommended. Such instruments are designed to effectively disrupt and eradicate mineralized deposits without undermining the integrity of the titanium surface or inducing surface microdamage that may enhance corrosion or bacterial colonization, and caution is needed as not all titanium curettes have less hardness that titanium implant alloys.
Submucosal instrumentation on the implant body should be approached with extreme care. Routine curettage in this area is not recommended unless there is clear, clinically justified evidence of hard deposit retention. Aggressive mechanical debridement of the submucosal titanium surface can disrupt the thin and critical titanium oxide passivation layer, resulting in the release of titanium microparticles. These particles have been demonstrated to provoke local pro-inflammatory responses, exacerbate tissue deterioration, and contribute to peri-implantitis progression. Hence, when submucosal decontamination is indicated, it should be conducted utilizing non-abrasive, evidence-based techniques that prioritize preservation of the implant’s surface integrity.
Step 2: Implant-associated risk factor management — highlighting residual cement
A vital part of the prevention and treatment of peri-implantitis is identifying implant-specific risk factors, which differ from those associated with natural dentition. Among these, residual excess cement has been consistently identified as one of the most deleterious contributors to peri-implant tissue inflammation and bone loss. Particularly in cement-retained implant restorations, retained submucosal cement, specifically resin-based materials, can induce a robust inflammatory response and act as a nidus for pathogenic biofilm formation.
Despite its clinical relevance, detection of residual cement presents a significant diagnostic limitation, especially when thin films are embedded submucosally or integrated within the mucosal seal. Visual inspection alone is frequently inadequate, and definitive identification usually mandates invasive methods, including endoscopic visualization and flap reflection. In this regard, the utilization of specialized diagnostic instruments becomes indispensable. This workflow incorporates the Impla-Safe Explorer (Salvin Dental, Charlotte, North Carolina), a purpose-designed instrument with a narrow, flexible tip tailored to navigate the unique anatomical contours of the implant-abutment-crown complex. Its design accommodates the “mushroom-like” emergence profile usually evident in implant prosthetics, permitting precise exploration at the critical junction where residual cement is most probable to accumulate. The approach relies heavily on improved tactile perception. During probing, the clinician should note subtle changes in resistance or elasticity. A typical “bounce” or deflection response felt upon contact may suggest the presence of residual cement. This non-invasive cue allows targeted cement retrieval efforts without requiring flap elevation, hence preserving soft tissue integrity.
Step 2B: Treatment protocol after identifying residual cement 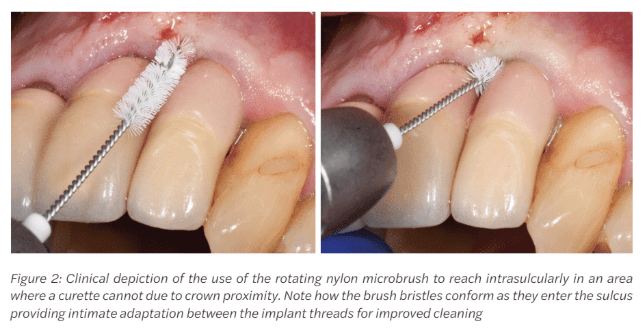
The eradication of excess cement alone can lead to the resolution of peri-implant mucositis or early peri-implantitis in nearly two-thirds of affected cases, underscoring its significance as a modifiable predisposing factor. Nonetheless, the method of removing excess cement must balance efficacy with preservation of the implant’s biological and structural integrity. Therefore, a single-stroke, conservative removal approach is emphasized. The objective is to disengage and extract the cement in one controlled motion, instead of repetitive scraping or scaling that could damage the peri-implant surface.
For this purpose, the Impla-Safe Cement Remover (Salvin Dental, Charlotte, North Carolina) is used. This instrument features an implant-specific sickle design with a micro-serrated working end, engineered to aid precise engagement of residual cement deposits, especially within the narrow submucosal interface at the crown-abutment junction. The micro-serrations offer mechanical interlocking with resin cement while minimizing friction against the titanium surface. The removal approach involves: (1) apical engagement of the cement margin with the serrated tip; (b) application of controlled coronal force in a single directional stroke; and (c) immediate re-evaluation employing tactile exploration to verify complete retrieval. Avoidance of multiple scaling strokes is crucial, as even seemingly minor mechanical trauma to the implant surface can lead to iatrogenic corrosion, particle shedding, and loss of surface biocompatibility.
Step 3: Sulcular irrigation with isotonic saline solution 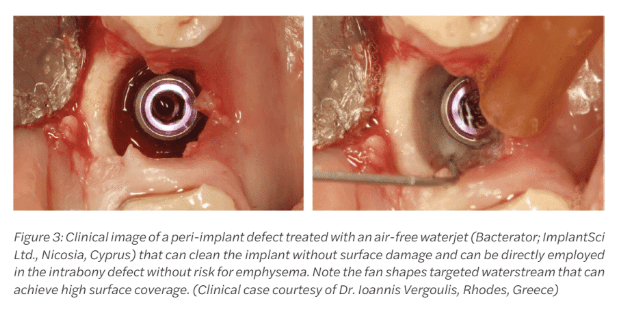
After removing the residual cement, the peri-implant sulcus should be thoroughly irrigated with sterile isotonic saline (0.9% NaCl). This step acts as an essential adjunct to the preceding mechanical intervention by facilitating the eradication of disrupted biofilm fragments, inflammatory exudate, free-floating bacterial colonies, and titanium microparticles that may have been released during instrumentation. The irrigation should be performed using a side-vented, blunt-tipped irrigation syringe to avoid undue trauma or pressure to the sulcular epithelium. Gentle flushing ensures that any loosely attached debris is physically displaced, especially from the complex micro-topographies of the implant collar and abutment interface, which are prone to harboring residual contaminants. In case the inflammation at the sites persists, such as in a case of refractory or recurrent peri-implant mucositis, the clinician can consider a diluted NaOCl irrigation with concentrations of no more than 1%, as this concentration ensures selective cytotoxicity. This means that it has antibacterial effects but does not compromise bone progenitor cells or affect regeneration. Importantly, chemotherapeutics with non-selective cytotoxicity should not be used on the implant threads as they get adsorbed and kill tissues cells such as fibroblasts and osteoblasts compromising peri-implant tissue attachment.
Step 4: Mechanical biofilm control with implant-specific, non-abrasive approaches
After initial debridement and sulcular irrigation, a critical next step in implant maintenance and peri-implant treatment is mechanical biofilm disruption using implant-safe, non-abrasive approaches. Given the delicate nature of the peri-implant interface and the risk of undermining the titanium surface integrity, biofilm control must be performed with precision tools that eradicate microbial deposits while preserving the implant’s passivated oxide layer.
The recommended approach involves utilizing titanium micropliers to hold a small piece of sterile gauze pre-soaked in 0.9% isotonic saline, followed by gentle “shoe-shine” strokes along the exposed implant collar and threads. This approach offers: (a) tactile control and visibility; (b) effective mechanical disruption of loosely attached biofilm; (c) minimal risk of particle shedding or surface modification; and (d) compatibility with titanium surfaces without causing iatrogenic microdamage. This gauze-based method enables clinicians to maintain mechanical precision and biocompatibility, especially in sites where complex thread geometries may harbor persistent microbial colonies. In instances where additional antimicrobial support is needed, agents used must be rigorously chosen for their selective or low cytotoxicity to host tissue, as mentioned above. Notably, chlorhexidine gluconate gets adsorbed on titanium when used locally and demonstrates cytotoxicity, which compromises tissue regeneration and should not be used in implant treatment when a pocket extending to the threads exists.
Alternatively, the recent consensus data suggest the use of mechanical non-abrasive means of cleaning to remove biofilm while maintaining implant surface integrity, such as: (a) polymer-based micro-brushes, engineered for implant use that provide contact-based mechanical debridement that is gentle enough to avoid titanium surface damage, while being structurally capable of disrupting biofilm matrices. These are specifically advantageous for complex or narrow prosthetic interfaces where gauze cannot sufficiently conform; and (b) waterjet irrigation systems, such as continuous-flow or pulsatile devices that help efficient eradication of detached biofilm and inflammatory byproducts from submucosal areas without direct mechanical friction.
Examples of mechanical contact maintenance instruments are the Impla-Safe®brush (Salvin Dental, Charlotte, North Carolina) and the Labrida BioClean™ Brush (Straumann AG, Andover, Massachusetts)14 both of which are mounted on reduction handpieces as rotating microbrushes. In contrast to rigid or metallic debridement instruments, soft polymer microbrushes comprise medical-grade polymer bristles, in the case of the BioClean brush enhanced with chitosan, particularly engineered to selectively interfere with biofilm while protecting the integrity of the implant surface. Clinical studies have indicated that the brush can substantially attenuate peri-implant mucosal inflammation and enhance clinical indices when utilized in combination with nonsurgical therapy, without causing noticeable alterations to the surface of titanium implants.14 Its non-metallic and flexible design renders it especially effective for cleaning exposed implant threads and complex prosthetic contours where traditional polymer tips or gauze may prove ineffective. Importantly, its utility has been reported as compatible, patient-friendly, and safe for multiple maintenance visits, in accordance with the principle of minimally invasive, surface-conserving peri-implant care.15
Both in vitro and human clinical evidence supports the use of non-metallic polymer microbrushes as an effective implant-safe method for biofilm disruption. A clinical trial showed that these brushes significantly reduced peri-implant mucosal inflammation while preserving the integrity of the titanium surface, with significantly better performance compared to titanium curettes.8 Their flexible, synthetic bristles are engineered to conform to complex implant geometries, allowing efficient access to narrow prosthetic interfaces that are difficult to clean with gauze alone. These findings suggest that polymer microbrushes may offer a gentle yet effective alternative to abrasive instrumentation in non-surgical peri-implantitis management.8
Beyond mechanical contact cleaning, new data suggests that mechanical non-contact cleaning with the use of air-free waterjet irrigation is a very promising and effective adjunct for peri-implant decontamination.6,16 An air-free waterjet system was employed in a preclinical study to deliver continuous saline flow without air infusion, minimizing the risk of subcutaneous emphysema while efficiently flushing biofilm and debris from the implant surface.16 Early results demonstrated significantly improved cleaning efficacy both in terms of bacterial and biofilm removal as compared to titanium brushes and curettes suggesting that air-free waterjet irrigation may optimize non-surgical peri-implantitis therapy beyond mechanical contact abrasive cleaning.16
In conclusion, according to the AO/AAP consensus on peri-implantitis, effective peri-implantitis management requires therapeutic strategies that preserve titanium surface integrity while addressing both microbial and material-driven inflammation.6 Emerging evidence underscores that abrasive instrumentation may exacerbate disease by releasing titanium particles, reinforcing the need for implant-specific, non-abrasive decontamination workflows. Clinicians should prioritize gentle mechanical protocols, targeted risk-factor control such as cement removal, and the use of surface-friendly biofilm disruption tools to support tissue stability and re-osseointegration. Integrating these principles into routine practice offers an evidence-driven approach for improving peri-implant health and long-term implant success.
Oral hygiene is a factor in peri-implant maintenance. Read this CE by Dr. Gregori M. Kurtzman and Debbie Zafiropoulos on the importance of the home care process. https://implantpracticeus.com/ce-articles/oral-hygiene-and-dental-implant-maintenance-part-1/
- Kotsakis GA, Black R, Kum J, Berbel L, Sadr A, Karoussis I, Simopoulou M, Daubert D. Effect of implant cleaning on titanium particle dissolution and cytocompatibility. J Periodontol. 2021 Apr;92(4):580-591. doi: 10.1002/JPER.20-0186. Epub 2020 Sep 11.
- Ahmed P, Bukhari IA, Albaijan R, Sheikh SA, Vohra F. The effectiveness of photodynamic and antibiotic gel therapy as an adjunct to mechanical debridement in the treatment of peri-implantitis among diabetic patients. Photodiagnosis Photodyn Ther. 2020 Dec;32:102077. doi: 10.1016/j.pdpdt.2020.102077. Epub 2020 Nov 4.
- Harrel SK, Wilson TG Jr, Pandya M, Diekwisch TGH. Titanium particles generated during ultrasonic scaling of implants. J Periodontol. 2019 Mar;90(3):241-246. doi: 10.1002/JPER.18-0230. Epub 2018 Nov 14.
- Fox SC, Moriarty JD, Kusy RP. The effects of scaling a titanium implant surface with metal and plastic instruments: an in vitro study. J Periodontol. 1990 Aug;61(8):485-90. doi: 10.1902/jop.1990.61.8.485.
- Mann M, Parmar D, Walmsley AD, Lea SC. Effect of plastic-covered ultrasonic scalers on titanium implant surfaces. Clin Oral Implants Res. 2012 Jan;23(1):76-82. doi: 10.1111/j.1600-0501.2011.02186.x. Epub 2011 Apr 13.
- Wang HL, Avila-Ortiz G, Monje A, Kumar P, Calatrava J, Aghaloo T, Barootchi S, Fiorellini JP, Galarraga-Vinueza ME, Kan J, Lin GH, Ravida A, Saleh MHA, Tavelli L; AO/AAP Consensus Participants; Rosen PS. AO/AAP consensus on prevention and management of peri-implant diseases and conditions: Summary report. J Periodontol. 2025 Jun;96(6):519-541. doi: 10.1002/JPER.25-0270. Epub 2025 Jun 12.
- Yen Nee W, Raja Awang RA, Hassan A. Effects on the Titanium Implant Surface by Different Hygiene Instrumentations: A Narrative Review. Cureus. 2022 Oct 30;14(10):e30884. doi: 10.7759/cureus.30884.
- Daubert D, Lee E, Botto A, Eftekhar M, Palaiologou A, Kotsakis GA. Assessment of titanium release following non-surgical peri-implantitis treatment: A randomized clinical trial. J Periodontol. 2023 Sep;94(9):1122-1132. doi: 10.1002/JPER.22-0716. Epub 2023 May 2.
- Safioti LM, Kotsakis GA, Pozhitkov AE, Chung WO, Daubert DM. Increased Levels of Dissolved Titanium Are Associated With Peri-Implantitis – A Cross-Sectional Study. J Periodontol. 2017 May;88(5):436-442. doi: 10.1902/jop.2016.160524. Epub 2016 Nov 18.
- Wilson TG Jr. Bone loss around implants-is it metallosis? J Periodontol. 2021 Feb;92(2):181-185. doi: 10.1002/JPER.20-0208. Epub 2020 Aug 13.
- Rosen PS. What Is an Effective Method for Treatment of Peri-implantitis? Compend Contin Educ Dent. 2020 Jul/Aug;41(7):378-383.
- Wilson TG Jr. The positive relationship between excess cement and peri-implant disease: a prospective clinical endoscopic study. J Periodontol. 2009 Sep;80(9):1388-92. doi: 10.1902/jop.2009.090115.
- Monje A, Amerio E, Cha JK, Kotsakis G, Pons R, Renvert S, Sanz-Martin I, Schwarz F, Sculean A, Stavropoulos A, Tarnow D, Wang HL. Strategies for implant surface decontamination in peri-implantitis therapy. Int J Oral Implantol (Berl). 2022 Sep 9;15(3):213-248.
- Wohlfahrt JC, Aass AM, Koldsland OC. Treatment of peri-implant mucositis with a chitosan brush-A pilot randomized clinical trial. Int J Dent Hyg. 2019 May;17(2):170-176. doi: 10.1111/idh.12381. Epub 2019 Feb 7.
- Khan SN, Koldsland OC, Roos-Jansåker AM, Wohlfahrt JC, Verket A, Mdala I, Magnusson A, Salvesen E, Hjortsjö C. Non-surgical treatment of mild to moderate peri-implantitis with an oscillating chitosan brush or a titanium curette-12-month follow-up of a multicenter randomized clinical trial. Clin Oral Implants Res. 2023 Jul;34(7):684-697. doi: 10.1111/clr.14078. Epub 2023 May 3.
- Jazaeri MS, Siddiqui DA, Tsai YC, Gabel K, Lorenzana Z, Kotsakis GA. Biofilm removal capacity and titanium surface integrity in non-abrasive versus abrasive peri-implantitis cleaning interventions. J Periodontol. 2025 Dec 10. doi: 10.1002/jper.11371. Epub ahead of print.
Stay Relevant With Implant Practice US
Join our email list for CE courses and webinars, articles and mores

