Drs. Yung-Ting Hsu and Hom-Lay Wang summarize and reveal management protocols for implant complications
There is no doubt that the advent of dental implants is a revolution in modern dentistry.
In addition to fixed and removable prostheses supported by natural teeth, patients are now offered implants for replacement of their missing teeth. Without sacrificing tooth structure, implants resemble natural teeth in both function and esthetics. Thus, more and more implants have been placed in the past decades. Like the occurrence of periodontal disease or caries on natural teeth, however, the presence of peri-implant complications has been rising in recent years.
What are implant complications?
From the authors’ point of view, implant complications can be categorized into three major types: biological, biomechanical, and esthetic implant complications. Similarly to periodontal disease, biological implant complications (ie, peri-implant diseases) present the inflammatory reactions on peri-implant tissues, including peri-implant mucositis, peri-implantitis, and implant loss.
The primary etiologic factors of biological implant complications are bacterial pathogens and impaired host immune response. Besides these, multiple factors have been linked with the presence of biological implant complications, such as a history of periodontal disease, inadequate oral hygiene, and so on. Residual cement and smoking have also been reported as the risk factors (Mombelli and Decaillet 2011; 2013).
On the other hand, mechanical overload is considered as the main cause of biomechanical implant complications (Misch, et al., 2005). Unlike natural teeth, dental implants contact supporting bone directly instead of the periodontal ligament (PDL). Without the cushion provided by the PDL, occlusal overstressing on dental implants tends to concentrate on crestal bone regions or implant prosthetic components and thereby causes biomechanical complications. Furthermore, other factors may also contribute to the occurrence of biomechanical overload, including inappropriate implant position, poor implant or prosthetic designs, and parafunction (Fu, et al., 2012; Hsu, et al., 2012).
Even though the implant survival rate is high in general, the presence of implant complications is not rare. Previous studies reported the incidence of peri-mucositis was approximately 50% (Roos-Jansaker, et al., 2006; Rinke, et al., 2011).
It is believed that this number was underestimated due to the reversibility of peri-mucositis (2013). For the complications caused by occlusal overload, Goodacre and co-workers reported several complications occurring in 1%-22% of implant-supported fixed prostheses (Goodacre, et al., 2003).
As for the occurrence of marginal bone loss, however, it varied from the definition/criteria used in different studies. Depending on the criteria, the prevalence of marginal bone loss ranged from 16.0%-36.6% (Roos-Jansaker, et al., 2006; Koldsland, et al., 2010).
In fact, these data are suggesting that it is about time to face the challenges of peri-implant complications and learn how to properly manage them to better serve our professional, as well as the patients whom we are treating.
How to manage biological and biomechanical implant complications?
People say, “An ounce of prevention is worth a pound of cure.”
To decrease the incidence of implant complications, it is important to have a comprehensive treatment plan and sound clinical performance both surgically and prosthetically. Regular implant maintenance is also essential after active therapy. Indeed, most of the implant biological complications are found during supportive therapy. The earlier the complication is diagnosed, the easier the clinician can fix the problem. The following section aims to suggest a flow chart about management of implant complications, which is summarized in Figure 1.

Examination
During implant maintenance, a thorough examination is the first step to prevent the existing peri-implant complications getting worse. The clinician can identify these complications by patients’ complaints, clinical examination, and radiographic assessment.
Clinically, probing around implants with light force (0.25 N) using conventional probes is allowed and helpful to detect peri-implant diseases in the early stage (Etter, et al., 2002; Heitz-Mayfield, et al., 2013).Probing depth and bleeding on probing (BOP), as well as gingival color alteration, may indicate the changes of peri-implant health and the severity of disease.
Checking occlusion and the integrity of prosthetic components is also helpful in recognizing possible biomechanical implant complications. Nevertheless, implant mobility is not considered as an effective indicator because it could only detect the differences in the late stage (2013). Besides, the changes to hard tissue can be investigated by using radiographic aids.
Conventional radiographic examina-tions, such as periapical films and vertical bitewings, are necessary for baseline and annual assessment. They can help discover the crestal bone level changes, or the presence of pathologic lesions. In spite of scattering effects, cone beam computed tomography (CBCT) scan may also provide the information for fenestration or dehiscence through its three-dimensional images. In some persistent cases of biological complications, clinicians and patients may benefit from microbiological analysis to select antibiotics adjunctive therapy.
Diagnosis
After examination, accurate diagnosis is the next step that guides us toward the direction of treatment strategies.
According to the recent American Academy of Periodontology (AAP) state-ment, peri-mucositis has been defined as an inflammatory reaction limited on soft tissue around implants, whereas peri-implantitis infects both soft tissue and supporting bone (2013). The signs of peri-implant disease include BOP, gingival redness, and possible suppuration (Lang and Berglundh 2011).
Biomechanical implant complications comprise the fracture or loosening of implant prosthetic components, early implant loss, and fracture of the implant body. Moreover, they share the same characteristics: progressive marginal bone loss, which may lead to implant loss in the late stage.
For those implants without a radio-graphic baseline, peri-implantitis may be diagnosed if the marginal bone loss is ³ 2 mm following biological bone remodeling (Sanz, et al., 2012).
It should be kept in mind that the signs of both biological and biomechanical implant complications may be combined in the same lesions due to the presence of multiple etiologic factors.
Management
Removal of etiologic factors and control of contributing factors are essential to stop disease progression. In other words, eliminating biofilms and related risk factors are the primary goal when treating biological implant complications.
In addition to adequate home/professional care and controlled systemic disease, smoking cessation should be discussed with patients prior to implant therapy.
For peri-implant mucositis, it is believed that non-surgical therapy using mechanical debridement is capable of controlling the inflammation and reducing probing pocket depth (Porras, et al., 2002; Trejo, et al 2006).
Non-surgical therapy also includes laser treatment and chemical antimicrobial agents (Heitz-Mayfield, et al., 2013).
As for the management of biomechanical implant complications, finding and removing the source of overstress are essential (Kim, et al., 2013).
Occlusal equilibration should be done prior to retightening the loosening prosthesis/abutment screw. The fracture prosthetic components should be replaced or repaired. Besides, occlusal bite splint is highly recommended for patients suffering from parafunction (Hsu, et al., 2012).
Treatment strategies vary in the management of marginal bone loss, depending on the morphology and severity of bony destruction.
For minor bony destruction (i.e., vertical bone loss £ 2 mm), non-surgical therapy, including adjunctive therapies, is recommended. Instead, surgical therapy is more effective in the treatment of bony destruction > 2 mm where that is still less than half of implant fixture length. Similarly to periodontal defects, regenerative surgery should only be considered for 2- or 3-wall intrabony defects.
Meanwhile, osseous resective surgery and implantoplasty are suggested for those defects presenting suprabony or non-regenerative destruction (Okayasu and Wang 2011; Muthukuru, et al., 2012; Renvert, et al., 2012).
If occlusal overload contributes to the marginal bone loss, occlusal splint should be considered after correction of occlusal problems (change/modification of implant prosthesis or selective occlusal adjustment).
In addition to conventional methods, various adjunctive therapies have been suggested in the treatment of peri-implantitis to decontaminate the implant surface, such as chemical, mechanical, and laser treatments and photodynamic therapy (PDT). A recent meta-analysis suggested that the use of local antibiotic delivery brought minor but significant improvement in the treatment of peri-implantitis (Muthukuru, et al., 2012).
On other hand, the adjunctive benefits of systemic antibiotics have not been investigated (Renvert, et al., 2012).
Laser therapy has also been used for the decontamination of the implant surface. Nevertheless, the efficacy has not been confirmed in either non-surgical or surgical treatments (Meyle 2012; Renvert, et al., 2012).
Implant removal should also be kept in mind as an option in the treatment of severe implant complications. For example, those implants with loss of osseointegration should be removed as soon as possible to prevent further inflammation and tissue loss. In implants with severe bony destruction — of more than 1/2 of implant length — or placed in inappropriate positions, removing the implant is a good option instead of saving implants with uncontrolled infection (Okayasu and Wang 2011; Aljateeli, et al., 2012).
In around 1% of cases presenting biomechanical implant complications, implant removal is the only option to treat implant body fracture (Hsu, et al., 2012).
Case report
This 50-year-old female, who is a former smoker, presented for implant maintenance. The implants were placed on the LL5 and LL6 about 6 months ago.
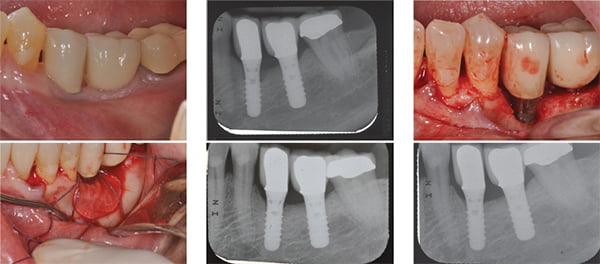
She reported the tenderness of peri-implant mucosa starting from a couple of weeks after the implant-supported crown delivery. In addition to localized gingival redness (Figure 2), the probing depth was 7 mm on buccal and distobuccal aspects of the LL5 implant with BOP and exudate discharge. Periapical film also showed marginal bone loss (Figure 3). Fortunately, there was no premature contact or signs of overloading when checking occlusion.
This lesion was thus diagnosed as a biological implant complication. To treat a peri-implant defect with >2 mm vertical bone loss, surgical therapy was planned. Due to the defect morphology (Figure 4), regenerative surgery was performed using allograft (enCore® mineralized allograft, Osteogenics Biomedical) and a collagen membrane (Pericardium, Zimmer Dental Inc.) (Figure 5). Significant regeneration was found at 3 months and 6 months post-operatively (Figures 6 and 7). After 6 months healing, the peri-implant mucosa returned to healthy status without BOP or exudate (Figure 8).
Conclusion

In conclusion, treatment strategies of peri-implant complications should be chosen based upon each individual case scenario. Comprehensive examinations together with accurate diagnoses are essential for the successful management of implant complications.
In spite of the complexity of the treatments, the prime objective of the treatment is to eliminate/control the etiologic factors and the contributing factors.
Depending on the severity of diseases, various approaches are available to manage biological implant complications, including non-surgical mechanical/chemi-cal debridement, regenerative surgery, and resective surgery with or without implantoplasty. Adjunctive therapies, such as antibiotics and laser, may be helpful in certain cases.
Meanwhile, occlusal equilibration should be achieved when treating biomechanical implant complications. Following repair or replacement of implant/prosthetic components, clinicians need to consider the occlusal bite splint therapy as a proactive precaution.
Nevertheless, implant removal should always be an option when the destruction is too severe to be repaired.
With the increasing need for implant placement, the occurrence of peri-implant complications is becoming a worldwide challenge. As implantologists in a new era, clinicians should have the knowledge of implant therapy, as well as associated peri-implant complications. More research is needed to further investigate peri-implant complications and their management. With the changing of these treatment approaches, it should be borne in mind that “a disease known is half-cured.”
This paper was partially supported by the University of Michigan Periodontal Graduate Student Research Fund.
- Clem DS, Cochran DL, Froum SJ, McAllister BS, Renvert S, Rosen PS, Wang H-L. American Academy of Perioodntology Report. Peri-implant mucositis and peri-implantitis: a current understanding of their diagnoses and clinical implications. J Periodontol. 2013;84(4): 436-443.
- Aljateeli M, Fu JH, et al. Managing peri-implant bone loss: current understanding. Clin Implant Dent Relat Res. 2012;14(Suppl 1):e109-118.
- Etter TH, Hakanson I, et al. Healing after standardized clinical probing of the perlimplant soft tissue seal: a histomorphometric study in dogs. Clin Oral Implants Res. 2002;13(6):571-580.
- Fu JH, Hsu YT, et al.. Identifying occlusal overload and how to deal with it to avoid marginal bone loss around implants. Eur J Oral Implantol. 2012;5(Suppl): S91-S103.
- Goodacre CJ, Bernal G, et al. Clinical complications with implants and implant prostheses. J Prosthet Dent. 2003;90(2):121-132.
- Heitz-Mayfield LJ, Needleman I, et al. Consensus Statements and Clinical Recommendations for Prevention and Management of Biologic and Technical Implant Complications. Int J Oral Maxillofac Implants. 2013 Aug 15.
- Hsu YT, Fu JH, et al. Biomechanical implant treatment complications: a systematic review of clinical studies of implants with at least 1 year of functional loading. Int J Oral Maxillofac Implants. 2012; 27(4):894-904.
- Kim Y, Oh TJ, et al. Occlusal considerations in implant therapy: clinical guidelines with biomechanical rationale. Clin Oral Implants Res. 2005;16(1):26-35.
- Koldsland OC, Scheie AA, et al. Prevalence of peri-implantitis related to severity of the disease with different degrees of bone loss. J Periodontol. 2010; 81(2): 231-238.
- Lang NP and Berglundh T. Peri-implant diseases: where are we now? Consensus of the Seventh European Workshop on Periodontology. J Clin Periodontol. 2011;38(Suppl 11):178-181.
- Meyle J. Mechanical, chemical and laser treatments of the implant surface in the presence of marginal bone loss around implants. Eur J Oral Implantol. 2012;5 (Suppl): S71-S81.
- Misch CE, Suzuki JB, et al. A positive correlation between occlusal trauma and peri-implant bone loss: literature support. Implant Dent. 2005;14(2):108-116.
- Mombelli A and Decaillet F (2011). The characteristics of biofilms in peri-implant disease. J Clin Periodontol 38 (Suppl 11):203-213.
- Muthukuru MA, Zainvi A, et al. Non-surgical therapy for the management of peri-implantitis: a systematic review. Clin Oral Implants Res. 2012;23 (Suppl 6):77-83.
- Okayasu K and Wang HL. Decision tree for the management of peri-implant diseases. Implant Dent. 2011;20(4):256-261.
- Porras R, Anderson GB, et al. Clinical response to 2 different therapeutic regimens to treat peri-implant mucositis. J Periodontol. 2002;73(10):1118-1125.
- Renvert S, Polyzois I, et al. (2012). Surgical therapy for the control of peri-implantitis. Clin Oral Implants Res. 2012;23(Suppl 6):84-94.
- Rinke S, Ohl S, et al. Prevalence of peri-implant disease in partially edentulous patients: a practice-based cross-sectional study. Clin Oral Implants Res. 2011;22(8):826-833.
- Roos-Jansaker AM, Lindahl C, et al. Nine- to fourteen-year follow-up of implant treatment. Part II: presence of peri-implant lesions. J Clin Periodontol. 2006; 33(4):290-295.
- Trejo PM, Bonaventura G, et al. Effect of mechanical and antiseptic therapy on peri-implant mucositis: an experimental study in monkeys. Clin Oral Implants Res. 2006;17(3): 294-304.
Stay Relevant With Implant Practice US
Join our email list for CE courses and webinars, articles and mores

