Dr. Ara Nazarian discusses implant treatment with fewer appointments
When a patient presents to your dental practice with questionable and/or non-restorable teeth requiring full-mouth extractions, the biggest concern is whether or not implants can be placed at the same surgical visit and, if so, will the patient be able to walk out with fixed teeth. Having an implant within your practice that allows you to load or progressively load so that these patients’ demands are met allows you to position your practice to a whole new level.
[userloggedin]
Of course, certain parameters must be met in order to facilitate this type of treatment. This includes, but is not limited to, the quality and quantity of bone, the presence of infection, the patient’s health, and the skills of the dental provider. Additionally, the selection of the most appropriate materials for the most ideal situation must be met.
 A patient presented to my practice for a consultation wanting to restore his dentition to proper form and function (Figure 1). He complained of generalized discomfort in these teeth due to the gross caries and periodontal disease that was readily apparent (Figure 2). There were several teeth in both arches that were already removed due to recurrent decay and/or fracture, which were previously restored with endodontic treatment, cores, and crowns. Also, there was hyper-eruption in certain areas of his posterior dentition, as well as a deep impinging bite in the anterior (Figures 3 and 4).
A patient presented to my practice for a consultation wanting to restore his dentition to proper form and function (Figure 1). He complained of generalized discomfort in these teeth due to the gross caries and periodontal disease that was readily apparent (Figure 2). There were several teeth in both arches that were already removed due to recurrent decay and/or fracture, which were previously restored with endodontic treatment, cores, and crowns. Also, there was hyper-eruption in certain areas of his posterior dentition, as well as a deep impinging bite in the anterior (Figures 3 and 4).
Planning
A CBCT scan using the CS 8100 3D (Carestream Dental) (Figure 5) was taken to accurately capture the information needed to properly treatment plan this case and ensuring the most ideal outcome, especially since the patient discussed his frustration with previous treatment that did not last very long or address his primary needs and requests.
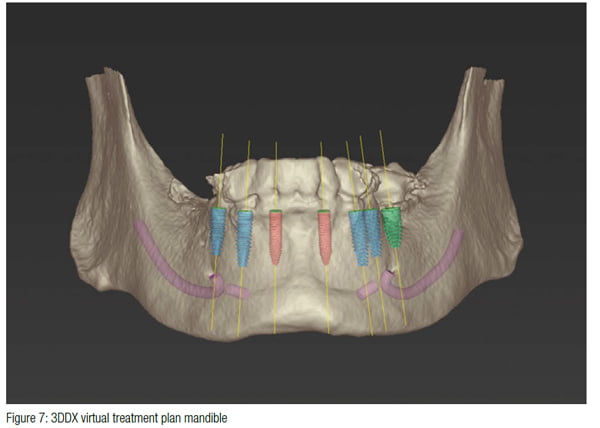
 To further develop a treatment plan, diagnostic model impressions were taken using Silginat® (Kettenbach), poured up and forwarded to the dental lab. These models were then mounted on an articulator (Stratos® 100, Ivoclar Vivadent®) for further analysis in order to meet the patient’s esthetic and functional needs. Additionally, a 3D virtual treatment plan was created with the assistance of 3DDX (3D Diagnostix.com) (Figures 6 and 7). The patient desired having fixed restorations supported by dental implants in both upper and lower arches.
To further develop a treatment plan, diagnostic model impressions were taken using Silginat® (Kettenbach), poured up and forwarded to the dental lab. These models were then mounted on an articulator (Stratos® 100, Ivoclar Vivadent®) for further analysis in order to meet the patient’s esthetic and functional needs. Additionally, a 3D virtual treatment plan was created with the assistance of 3DDX (3D Diagnostix.com) (Figures 6 and 7). The patient desired having fixed restorations supported by dental implants in both upper and lower arches.
 Financing options using a third-party payment option (Lending Club®) were discussed with the patient. This discussion was a very important part of facilitating acceptance of his care since it made the cost of treatment more feasible.
Financing options using a third-party payment option (Lending Club®) were discussed with the patient. This discussion was a very important part of facilitating acceptance of his care since it made the cost of treatment more feasible.
The implants utilized in this case were OCO Biomedical’s Engage™ dental implants. These implants are known for their unchallenged high implant stability at placement, which is a critical success factor in these immediate load cases. With the combination of their patented Bull Nose Auger™ Tip and Mini Cortic-O Thread™, the Engage™ implant system offers practitioners a bone level implant with high initial stability for selective loading options.
 The Engage™ implant is self-tapping for an enhanced mechanical lock in the bone. The Bull Nose Auger™ Tip will not proceed any deeper than the initial pilot drill preparation locking into the base of the osteotomy. Engage™ implants have a proprietary surface treatment designed to increase the surface area of the implant for optimal bone ingrowth and stability.
The Engage™ implant is self-tapping for an enhanced mechanical lock in the bone. The Bull Nose Auger™ Tip will not proceed any deeper than the initial pilot drill preparation locking into the base of the osteotomy. Engage™ implants have a proprietary surface treatment designed to increase the surface area of the implant for optimal bone ingrowth and stability.
 Once the teeth were extracted, the tissue was reflected in order to get the surgical guide seated and fixed with its respective retention pins. Using this universal surgical guide provided by 3D Diagnostix, the sites for the implants were initiated with a designated 1.8-mm pilot drill from the OCO Biomedical Guided Kit (Figure 8), utilizing the Mont Blanc® surgical handpiece and Aseptico® surgical motor (AEU 7000) at a speed of 1,200 rpm with copious amounts of sterile saline. Sequential osteotomy formers from the OCO Biomedical Guided Kit were then used to shape the final osteotomies. Once the osteotomies were complete, an implant driver was used to place the dental implants until increased torque was necessary (Figure 9). The ratchet wrench was then connected to the adapter and the implants torqued to final depths reaching a torque level of about 40-50Ncm.
Once the teeth were extracted, the tissue was reflected in order to get the surgical guide seated and fixed with its respective retention pins. Using this universal surgical guide provided by 3D Diagnostix, the sites for the implants were initiated with a designated 1.8-mm pilot drill from the OCO Biomedical Guided Kit (Figure 8), utilizing the Mont Blanc® surgical handpiece and Aseptico® surgical motor (AEU 7000) at a speed of 1,200 rpm with copious amounts of sterile saline. Sequential osteotomy formers from the OCO Biomedical Guided Kit were then used to shape the final osteotomies. Once the osteotomies were complete, an implant driver was used to place the dental implants until increased torque was necessary (Figure 9). The ratchet wrench was then connected to the adapter and the implants torqued to final depths reaching a torque level of about 40-50Ncm.
 A baseline ISQ reading was taken of these implants utilizing the Osstell ISQ unit (Figure 10). Since the initial readings were all around 70, and the quality of bone after leveling was good, temporary abutments (OCO Biomedical) were tightened into the Engage (OCO Biomedical) dental implants and prepped with copious amounts of water for immediate provisionalization.
A baseline ISQ reading was taken of these implants utilizing the Osstell ISQ unit (Figure 10). Since the initial readings were all around 70, and the quality of bone after leveling was good, temporary abutments (OCO Biomedical) were tightened into the Engage (OCO Biomedical) dental implants and prepped with copious amounts of water for immediate provisionalization.
 Any residual areas around the implants or in the sockets were grafted with a cortical mineralized and demineralized bone grafting material to optimize the area for regeneration. Primary closure was achieved by suturing the tissue with resorbable sutures.
Any residual areas around the implants or in the sockets were grafted with a cortical mineralized and demineralized bone grafting material to optimize the area for regeneration. Primary closure was achieved by suturing the tissue with resorbable sutures.
The prefabricated immediate provisional restorations were tried in to ensure a passive fit over the temporary abutments. Once confirmed, rubber dam material was placed to avoid the restoration from locking on during the relining procedure with Visalys® Temp (Kettenbach) temporary material. After the material polymerized, the immediate provisional restoration was removed, and any access material was removed with the Torque Plus (Aseptico) lab handpiece and acrylic bur (Komet). Once trimmed and polished, the provisional restorations were seated with Temp-Bond™ Clear (Kerr Dental) (Figure 11).
Seven days postoperatively, the patient returned with very little discomfort, swelling, or bruising. He was very pleased with his new upper- and lower-fixed provisional restorations (Figure 12). Now that the patient was no longer anesthetized, the occlusion was checked again to confirm there were no interferences in lateral and protrusive movements. The next step in his treatment would consist of full arch impressions for the definitive restorations approximately 4-5 months postoperatively.
Conclusion
Having the ability to take a patient from start to finish in a fewer amount of appointments within your practice allows you to position yourself as a provider that can fulfill your patient’s surgical and restorative needs. With the proper training and appropriate materials, a dental provider may provide extraction, grafting, and implant placement within one appointment at one location. Not only does this allow you to reduce the amount of visits for the patient, but this type of service also helps maintain the cost to the patients since they are not seeing multiple dental providers. Most importantly, this enables the dental provider full control of the surgical and prosthetic outcome. Depending on the patient’s desires, the clinical conditions of the oral environment present, and the skills of the provider, a dentist may choose to extract teeth, level bone, and graft with guided dental implant placement within his/her dental practice.
 Ara Nazarian, DDS, DICOI, maintains a private practice in Troy, Michigan, with an emphasis on comprehensive and restorative care. He is a Diplomate in the International Congress of Oral Implantologists (ICOI) and the director of the Ascend Dental Academy. He has conducted lectures and hands-on workshops on esthetic materials, grafting, and dental implants throughout the United States, Europe, New Zealand, and Australia.
Ara Nazarian, DDS, DICOI, maintains a private practice in Troy, Michigan, with an emphasis on comprehensive and restorative care. He is a Diplomate in the International Congress of Oral Implantologists (ICOI) and the director of the Ascend Dental Academy. He has conducted lectures and hands-on workshops on esthetic materials, grafting, and dental implants throughout the United States, Europe, New Zealand, and Australia.
Stay Relevant With Implant Practice US
Join our email list for CE courses and webinars, articles and mores

