Drs. Lyndon F. Cooper and Ghadeer N. Thalji present a simplified approach to divergent implant placement

Dental implant therapy for the edentulous mandible is highly successful when measured at the level of the dental implant. When component and prosthetic complications are considered, recent systematic reviews suggest that component and prosthesis complications occur frequently. Many of these complications are related to prosthesis design and have been attributed to the cantilever designs that impose significant bending moments and stress on the prostheses and components. The intentional divergence of implants from mutually parallel placement restricted to the parasymphyseal mandible has been proposed (Malo, et al., 2003) and has been recently substantiated by a retrospective evaluation revealing greater than 98% implant success (Malo, et al., 2011).
Educational aims and objectives
This article aims to illustrate the alternative use of conical interface abutments to simplify the construction of mandibular implant-supported fixed dentures (ISFD) supported by four implants with intended divergence.Expected outcomes
Implant Practice US subscribers can answer the CE questions on the quiz to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
- Realize that the use of conical-design abutments permits the intentional displacement of implants in non-parallel orientations without adding complexity to the required components for restoration.
- Realize that the placement of abutments of strength and utility enables the clinical management of the prosthesis at a tissue or supratissue level.
- Recognize the option of a simplified approach to divergent implant placement.
- Identify the process of implant placement for a patient with a complicated type of edentulous mandible.

The distal displacement of the terminal implants supporting mandibular implant-supported fixed dentures (ISFD) requires the use of abutments that geometrically reconcile the nonparallel arrangement of the implants and permit relative parallelism of the abutments. The aim of this case report is to illustrate the alternative use of conical interface abutments to simplify the construction of mandibular ISFD supported by four implants with intended divergence.
Diagnosis and treatment plan
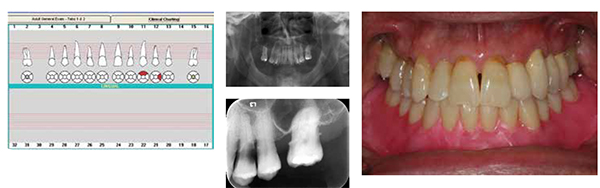
A 57-year-old male presented for treatment of mandibular edentulism. Clinical examination revealed a non-restorable, carious maxillary left canine and first premolar tooth and the linguoversion of the maxillary left lateral incisor (Figures 1A-1C). After discussion of options for treatment of mandibular edentulism that included a conventional denture, an implant-retained overdenture, and an implant-supported fixed prosthesis, the patient selected rehabilitation by four implants supporting a mandibular ISFD constructed of titanium alloy and resin veneer.

Treatment planning was performed using information gathered from the clinical chart, mounted radiographs, and the panoramic radiograph (Figures 2A-2C). A diagnostic waxing was performed to reveal the proposed restoration of the maxillary left lateral incisor and replacement of the maxillary right first premolar using a fixed dental prosthesis. A mandibular denture setup was waxed to characterize the position of teeth for the proposed interim denture and final prosthesis (Figure 3). The Class III skeletal relationship was adapted to a Class I tooth arrangement.

After reviewing treatment and obtaining informed consent, additional diagnostic measures for the surgical treatment were performed. The mandibular denture was flasked and processed in heat polymerizing resin (Lucitone® 199, Dentsply) using a conventional compression technique. Thereafter, the mandibular denture was duplicated using a radiopaque resin (Biocryl-X radiopaque acrylic resin, Great Lakes Orthodontics) polymerized in a custom laboratory putty mold (Figures 4A-4B).

A cone beam CT image was made of the patient wearing this radiographic template, and the DICOM files were imported into planning software (Dentsply Implants). Four implants were located within the para-symphyseal mandible and in relationship to the visualized denture teeth (Figure 5A). The implant selection and placement was performed to account for primary stability and osseointegration, restorative dimension, and minimal cantilever length for the available distribution of the implants. The targeted planning goal was to assure that there were at least four implants of >10 mm length, >10 mm of restorative dimension, and >10 mm of anterioposterior implant distribution (English 1990; Rangert, et al., 1989) to permit a cantilever of one premolar and one molar tooth (approximately 15 mm). Achieving these goals required distal angulation (Figure 5B) of the terminal implants and an alveoloplasty to assure adequate restorative dimension.
Surgical treatment
Four implants (OsseoSpeed™ TX, 4.0S x 11mm at the LL4, LR2, and LR4 sites, and a 3.5S x 11mm Dentsply Implants at the LL2) were placed in the parasymphyseal mandible. Under local anesthesia, a mucoperiosteal flap was elevated from the left molar region to the right molar region of the mandible. An alveoloplasty was performed from the left premolar region to the right premolar region with removal of approximately 4 mm of crestal bone (Figure 6A). This resulted in the exposure of a mandibular alveolar crestal shelf of approximately 5 mm-6 mm in buccolingual width and afforded an additional 3 mm of restorative dimension. Using the radiographic template with appropriately oriented 2.5 mm diameter guides drilled for surgical orientation, 2.0 mm osteotomies were placed to 4 mm-5 mm depth through the template. After affirming the proper orientation of the four osteotomies, each osteotomy was sequentially enlarged to 11.0 mm x 3.7 mm for sites LL4, LR2, and LR4 and 11.0 mm x 3.2 mm for the LL2 according to the implant manufacturer’s recommended protocol (Figure 6B). Subsequently, 11.0 mm x 4.0 mm or 11.0 mm x 3.5S implants were placed into each osteotomy with primary stability (Figure 6C).

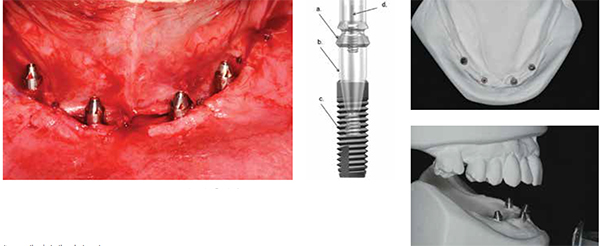
Next, a conical interface abutment (Uni-Abutment, Dentsply Implants) was placed with hand torque into each of the four implants, and the mucosa was sutured circumferentially to each of the abutments (Figures 7A-7B). On each of the 20º conical interface abutments, machined-titanium temporary cylinders (Dentsply Implants) were placed with hexed bridge screws using finger pressure only. The access chambers of the cylinders were filled with VPS impression material to exclude acrylic resin. The complete denture was relieved to accommodate the temporary cylinders but with the full extension of the flanges intact.
Upon closure, the coincidence of the denture maximum intercuspation at centric relation confirmed that the temporary cylinders did not displace the denture orientation. At that position, each of the four temporary cylinders was incorporated into the denture using autopolymerizing acrylic resin with a rubber dam placed beneath the cylinders to protect the surgical site. The conversion prosthesis was then refined by removal of the flanges and eliminating the cantilever extension beyond the mesial cusps of the first molar. The prosthesis was delivered using four hex bridge screws, and the access holes were filled with VPS material.
Restorative treatment
After 8 weeks of healing, the patient returned for an impression of the abutments to construct the final prosthesis. First, an inter-occlusal record using the existing interim prosthesis at centric relation was taken. Then, the interim conversion prosthesis was removed, the stability of the implants and abutments was verified, and an impression of the implant abutments made at the level of the 20º conical interfaces using a stock tray and VPS impression material.

The master cast was poured to incorporate 20º conical interface analogues without a soft tissue moulage (Figures 8A-8B). A verification index was fabricated using four impression copings and acrylic resin (GC Pattern Resin™) (Figure 9). The verification index was tested clinically to confirm the accuracy of the master cast. The interim conversion prosthesis and the interocclusal record were used to mount the mandibular master cast in correct relationship to the maxillary cast. A shade was taken for fabrication of the final prosthesis using nanohybrid composite/resin teeth (SR Phonares® II, Ivoclar Vivadent®).
Laboratory procedures
The fabrication of the mandibular prosthesis required CAD/CAM design and milling of a titanium alloy bar. For this process, the dentist must provide the laboratory or milling center with a) a master cast, b) a verification index that confirmed the position of the analogues in the cast, c) a copy of the mandibular denture, or an impression of the existing conversion prosthesis. No articulator is required for the CAD/CAM design and manufacture of the milled framework.
The design of the framework should take account of the position of the teeth and should address concerns of imposed function. In this case, the framework design utilizes an effective “Y” design to provide resistance to deformation and strength (Figures 10A-10B). The regions of the framework distal to the screw access areas are bolstered to account for known stresses that accumulate in this area of cantilever bars. Note that the design is within the contours of the scanned denture and should not interfere with the prosthetic teeth.
The distal inclination of the implants does not impede the use of simple abutments as these abutments possess 20º conus interfaces for the framework. In most cases, displacement of the implants leading to access screws exiting the first or second premolar region involves approximately 25º of angulation between the two implants and is easily reconciled by 40º of mutual angulation between two 20º conus interface abutments (Figure 11). There exists no need for an angled abutment component. There is no need to assess the fit of the framework due to the accuracy of manufacture and the provision of the verification index.


Upon delivery of the framework, it is transferred to the articulator and nanohybrid composite/PMMA teeth (SR Phonaris II, Ivoclar Vivodent) were arranged in baseplate wax for try-in and final evaluation (Figure 12A).
In this particular case, one implant was placed facial to the anterior tooth plane. This is attributable to the conversion of a skeletal Class III relationship to a Class I dental relationship.
One approach to solving the interference of the screw access with the esthetic aspects of the incisor tooth is to construct the acrylic veneer prosthesis with the denture tooth deleted from the position of the offending screw access during processing. This approach was taken in design and implementation of prosthesis construction (Figure 12B).
Metal frameworks for implant-supported fixed dentures typically require opaquing of the metal color. This can be done using different methods that include adhesive and non-adhesive application of materials. Another innovative approach is the anodization of the titanium alloy metal substrate to a pink hue (Figures 13A-13B). This technology is commercially available (AccuFrame® Plus, Cagenix™, Memphis, Tennessee) and was applied in this instance.

Following tooth try-in and acceptance by the patient, the fabrication of the ISFD was completed by conventional processing that included tinting of the acrylic resin base using white, red, and melanin shading acrylics (Kayon® denture stain kit, Englewood, New Jersey). Just prior to flasking of the prosthesis, the lateral incisor tooth interfering with bridge screw access was removed from the wax-up (Figure 14).
The interface between the tooth and the baseplate wax was refined, and then the waxed denture was finally flasked in plaster. The acrylic resin base and teeth were polymerized and de-flasked, and the prosthesis without the lateral incisor tooth was revealed (Figures 15A-15C). The lateral incisor tooth was easily fit to the recipient acrylic resin housing the screw access, and the entire prosthesis was finally polished.

Delivery and follow-up care
The processed denture was delivered using four bridge screws tightened to 15Ncm. Prior to closing the screw access and placement of the lateral incisor tooth, an occlusal photograph was made and given to the patient. All hex bridge screws were covered with cotton pellets. The lateral incisor tooth was fit into the recipient acrylic resin housing and bonded into place using ProTech Plus® self-cure hard reline and repair acrylic resin (ProTech Professional Products). The screw access hole exiting the pink denture resin was filled with pink-fibered triad resin (Dentsply), and the screw access holes exiting the premolar teeth were filled with shade A3.5 composite resin (Kerr, Orange, California). These surfaces were covered with Vaseline®, smoothed with a gloved finger, and then light polymerized in order to avoid polishing. The occlusion was verified using articulating paper visualization and bilaterally symmetric contacts in centric occlusion as demonstrated using shimstock (Figures 16A-16E).

Summary
The use of conical-design abutments permits the intentional displacement of implants in nonparallel orientations without adding complexity (additional screws, specific angled components, or custom abutments) to the required components for restoration. The 20º configuration illustrated here offers resistance along the abutment/prosthesis interface that contributes to stability of bridge screws.
The use of CAD/CAM manufacture of frameworks does not preclude the use of individual abutments in construction. The placement of abutments of strength and utility enables the clinical management of the prosthesis at a tissue or supratissue level.
References
- Maló P, Rangert B, Nobre M. “All-on-Four” immediate-function concept with Brånemark System implants for completely edentulous mandibles: a retrospective clinical study. Clin Implant Dent Relat Res. 2003;5 Suppl 1:2-9.
- Malo P, de Araújo Nobre M, Lopes A, Moss SM, Molina GJ. A longitudinal study of the survival of All-on-4 implants in the mandible with up to 10 years of follow-up. J Am Dent Assoc. 2011;142(3):310-320.
- English CE. Critical A-P spread. Implant Soc. 1990;1(1):2-3.
- Rangert B, Jemt T, Jörneus L. Forces and moments on Branemark implants. Int J Oral Maxillofac Implants. 1989;4(3):241-247.
Stay Relevant With Implant Practice US
Join our email list for CE courses and webinars, articles and mores
