Dr. Ashok Sethi examines how the advent of technology has improved the options available for patients and clinicians alike

Human evolution is progressing at an exponential rate — something that is reflected in all human endeavors, including implant dentistry. This article aims to address the changes that have taken place within this field, consider the way they have impacted the way we work, and look at the benefits this has brought for our patients.
In modern implant dentistry, conceiving the end result before embarking on treatment has become easier, making it possible for both the patient and clinician to have an idea of the direction in which they are travelling. This article will specifically address the application of three-dimensional imaging, stereolithography, and CAD/CAM technology in the current practice of implant dentistry. Treatment carried out in stages, as well as the immediate replacement of failing teeth will be addressed.
Backward planning (forward thinking)
Conceiving the end result before embarking on treatment requires a number of stages, both technical and clinical. The key is in starting off with a realistic diagnostic preview (Figure 9) and transferring this information from one stage to the next and between the laboratory casts and the mouth. Three-dimensional imaging coupled with an interactive software program (SIMPLANT®, Leuven, Belgium; DENTSPLY Implants) greatly increases the accuracy and predictability with which the treatment can be completed (Sethi and Kaus, 2012).

Educational aims and objectives
This article aims to address the application of three-dimensional imaging, stereolithography,
and CAD/CAM technology in the current practice of implant dentistry.
Expected outcomes
Implant Practice US subscribers can answer the CE questions to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
- Realize how new technologies have improved available treatment options.
- Recognize how position and the dimensions of the implants can be decided upon with technology.
- Identify how an interactive software program can greatly increase the accuracy and predictability with which the treatment can be completed.
- Realize how to utilize diagnostic imaging and transfer of tooth position data for immediate implant patients.
- Realize how CBCT, stereolithography, and CAD/CAM are key elements in the immediate implant process.
Immediate replacement of failing teeth
Staged treatment is highly predictable. However, recent observations and developments in surface technologies have made it equally predictable to place implants immediately and bring them into function at the same time. This is also very attractive for patients because of the reduction in the number of surgical appointments. Most importantly, this provides the patient with a very attractive option of having the failing teeth removed and the new teeth implanted at the same time, albeit with a provisional restoration. The same process of diagnostic imaging and transfer of tooth position data can be carried out for a patient with failing teeth where there is a need for immediate placement of these teeth with implants.

The position and the dimensions of the implants required for rehabilitation of the patient can be decided upon within the SIMPLANT program derived directly from CBCT data. This information can be transferred to a drill guide, which will enable the placement of the implants in the correct position and depth. This is facilitated by the use of stereolithographic models made directly from CT scan data. This, of course, enables the fabrication of the transitional restorations directly on the stereolithographic models. At the same time, selection of the abutments can be carried out based on the selected tooth position.
CAD/CAM technology

The first stage is to construct an accurate cast of the abutments in the patient’s mouth (Assif, et al., 1996; Assif, et al., 1999). It is then possible to scan the cast with the abutments, using a digital scanner. At the same time, the diagnostic preview (waxup) indicating the position of the planned teeth needs to be scanned.
Once the desired tooth position and the abutment position and shape have been scanned, it is possible to fabricate a prosthetic framework by milling it from a number of materials. These may be titanium, zirconium oxide, or a chrome-cobalt alloy. Porcelain or acrylic can then be veneered onto the framework.
Case studies
The cases studies illustrate how three-dimensional imaging, stereolithography, and CAD/CAM technology can be put in practice in different clinical situations.

Case 1 (Figures 1-5) depicts the management of a patient whose medical condition indicated the reduction of the number of interventions to a minimum.
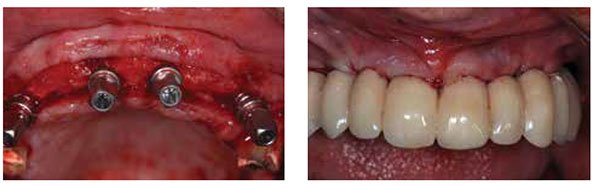
Case 2 (Figures 6-13) depicts the management of a patient with failing teeth who required a change in the appearance as well as the occlusal scheme to achieve a better esthetic and functional outcome.
Case 3 (Figures 14-20) depicts the fabrication of a framework using CAD/CAM technology, which enables a more accurate fit to be achieved than a framework made by conventional casting technology (Takahashi and Gunne, 2003).




References
- Assif D, Marshak B, Schmidt A. Accuracy of implant impression techniques. Int J Oral Maxillofac Implants. 1996;11(2):216-222.
- Assif D, Nissan J, Varsano I, Singer A. Accuracy of implant impression splinted techniques: effect of splinting material. Int J Oral Maxillofac Implants. 1999;14(6):885-888.
- Sethi A, Kaus T. Practical Implant Dentistry. The Science and Art. 2nd ed. London: Quintessence Publishing Co. Ltd.; 2012.
- Takahashi T, Gunne J. Fit of implant frameworks: an in vitro comparison between two fabrication techniques. J Prosthet Dent. 2003;89(3):256-260.
Stay Relevant With Implant Practice US
Join our email list for CE courses and webinars, articles and mores
