Educational aims and objectives
This self-instructional course for dentists aims to discuss appropriate management of ingestion or aspiration of foreign bodies during implant placement.
Expected outcomes
Implant Practice US subscribers can answer the CE questions by taking the quiz to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
- Identify some of the etiology behind the ingestion or aspiration of foreign bodies during implant placement.
- Recognize some characteristics of ingestion of objects into the gastrointestinal tract during implant placement.
- Recognize some characteristics of objects aspirated into the lungs during implant placement.
- Realize some clinical strategies to avoid ingestion or aspiration of objects during dental implant procedures.
- Recognize some immediate symptoms in determining if the foreign body was aspirate
Dr. Randolph Resnik offers several options for handling the serious complication of ingestion or aspiration of implant components.
Dr. Randolph R. Resnik discusses solutions for this unexpected and potentially life-threatening situation
Introduction
In the literature, there is an abundance of case reports and clinical studies describing the ingestion or aspiration of foreign bodies such as teeth, orthodontic brackets, retainers, burs, crowns, posts, impression material, endodontic files, and syringe tips. Most recently, an ever-increasing complication associated with implant procedures is the loss of dental implant components (implants, abutments, screws, attachments, etc.) in the oropharynx resulting in ingestion or aspiration. Unfortunately, these foreign objects can be of various sizes and shapes, which may lead to significant morbidity from displacement in the gastrointestinal (GI) or the respiratory tract. Therefore, when this complication occurs in an office setting, the implant clinician must be well-informed on the appropriate management of the complication to avoid serious life-threatening and medicolegal issues.
Etiology
Due to the small and atypical size of implants, abutments, screws, drivers, and other implant components, this complication may easily occur at any time during implant procedures (surgical and prosthetic). Implant procedures are highly susceptible to these complications because of the difficulty in handling of the small implant instruments and components that are often slippery due to saliva or blood. Most implant procedures, either surgical or prosthetic, are completed in a supine or semi-recumbent position, which may predispose to ingestion or aspiration. In addition, other contributing factors include the use of local anesthesia (loss of gag reflex), oral or intravenous sedation, unexpected patient movements, poor access and visualization, limited openings, and unexpected detachment of implant components.
When an object is lost in the oropharynx, there exist two possibilities: patients may swallow the foreign object into the stomach or aspirate the foreign body into the lungs. Clinical studies evaluating the prevalence of this complication have shown that approximately 80% of objects lost are ingested into the GI system, and 20% are aspirated into the lungs.1
Ingestion
In most cases, ingested objects into the gastrointestinal tract usually result in no immediate symptoms from the patient. Approximately 90% of ingested objects usually pass through the gastrointestinal tract uneventfully in 4 to 6 days; however, irregularly shaped objects have been known to take up to 4 weeks. Studies have shown that objects will pass unimpeded through the gastrointestinal system (GI) in 80% of cases if the object is less than 3 cm.2
The management of ingested objects most commonly depends on the risk for GI perforation and will usually result in either (1) periodic monitoring or (2) removal (via endoscopy or laparotomy).3 Periodic monitoring will most commonly involve a radiographic survey to ascertain the movement of the object. The perforation rate in the GI system is directly related to the size and sharpness of the object where sharp, pointed, and elongated objects have been reported to have an approximate 15% – 35% perforation rate.4
Aspiration
In most cases, any foreign object that is aspirated into the lungs should be treated as a medical emergency. The foreign body could be located anywhere along the tracheobronchial tree; however, the right bronchus is the most common site because of its more vertical and wider anatomic configuration in comparison to the left bronchus.5 Usually, the patient will be symptomatic, exhibiting signs of laryngotracheal obstruction such as dyspnea, coughing, wheezing, stridor, or cyanosis. If airway obstruction is present, the clinician should immediately initiate CPR/emergency airway obstruction protocols.
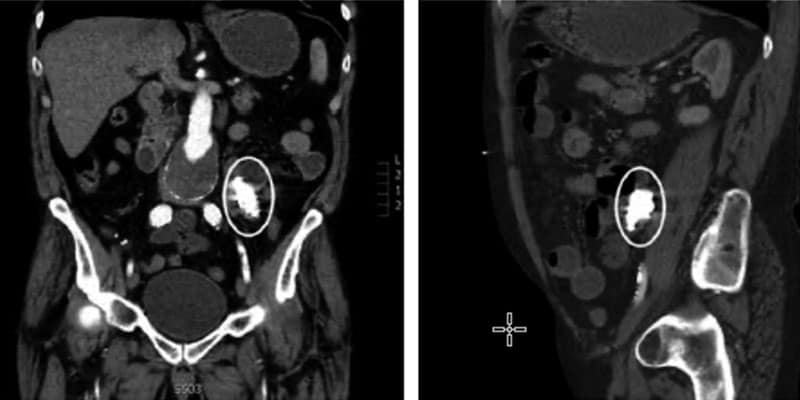
Ideally, after location is confirmed, retrieval is necessary most commonly with flexible or rigid bronchoscopy. Bronchoscopy has been shown to be 99% effective in the removal of foreign objects; however, 1% require surgical retrieval. Long term retention of the foreign body in the respiratory system can be life-threatening resulting in possible pneumonia, atelectasis, pneumothorax, hemorrhage, or lung abscess (Figures 1 and 2).

Prevention
Numerous clinical strategies exist to avoid ingestion or aspiration of objects during dental implant procedures. It is imperative the dental implant clinician integrate specific prevention treatment techniques and protocols to minimize the possibility of aspiration or ingestion of implant components. Unfortunately, there is no one technique that will guarantee this complication from occurring; however, extreme caution should always
be exercised.
Techniques to prevent swallowing or aspiration include:
- Patient positioning: For implant procedures with an increased risk of ingestion or aspiration, the patient should be seated in a more upright position instead of supine position.
- Throat packs or pharyngeal screens: The easiest and most common technique to avoid ingestion or aspiration is the use of 4 x 4 surgical gauze. The gauze should be opened and positioned in the oral cavity distal to the area of treatment. A 2 x 2 gauze should never be used, as saliva or blood impregnation may lead to the gauze being aspirated or ingested due to its small size (Figure 3).
- Ligatures: Floss or suture material should be tied to any possible implant component so easy retrieval may be completed if an object is lost into the oropharynx (Figure 4).
- Special insertion tools: Use of special screw insertion tools and drivers which allow for manipulation outside of the oral cavity (Figure 5).
- High-vacuum suction: Can be used with a large aspirator if the foreign body is easily accessible.
- Curved Kelly hemostat: For retrieval of objects in oropharynx, ideally the hemostat should be located in the operatory for easy access (Figure 6).
- O-ring replacement: Implant com-ponents containing O-rings should periodically be evaluated for signs of wear or material fatigue and replacement when warranted (Figure 7).
- Surgical Gloves: Because of blood and saliva, it is not uncommon for surgical gloves to become slippery. Therefore, periodic glove replacement will prevent this complication.


Treatment
If a foreign object is lost in the oropharynx, the patient should be instructed to not immediately sit straight up, as this will ensure the ingestion or aspiration of the instrument. The patient should ideally turn to the side and attempt to “cough” the implant component up. If the foreign object is visible to the implant clinician, attempts to retrieve it with curved hemostats or a high-volume suction is indicated. However, care should be exercised to prevent further displacement deeper into the oropharynx.
It is imperative that clinicians have a strong understanding of the etiology and treatment of this complication along with integrating preventive protocols into their office.
If the instrument is lost, immediate symptoms usually are a good indicator in determining if the foreign body was aspirated or ingested. If the patient exhibits coughing, wheezing, pain, and cyanosis symptoms, an immediate medical emergency protocol should be initiated, as this is indicative of aspiration. If the patient is asymptomatic, which usually indicates ingestion, it is mandatory the patient be referred to their physician or emergency room for immediate radiographs. Radiographic examination (usually chest and abdomen radiograph) is necessary for diagnosis of the location, size, and shape of the foreign body, as well as the need for immediate medical intervention
Conclusion
In summary, any object or instrument placed into the oral cavity during a dental implant procedure may be ingested or aspirated. Although this has been characterized as an infrequent complication in the office setting, with the recent popularity of implant procedures, it is definitely an emerging problem and complication. Clinicians should have a strong understanding of the etiology and treatment of this complication along with integrating preventive protocols into their office. Radiographic imaging and medical attention is critical in the determination of the foreign object’s location and the required course of medical treatment. If this complication is not treated properly in a timely fashion and managed appropriately, life-threatening consequences may result.
Author Info
 Randolph R. Resnik, DMD, MDS, is a leading clinician, educator, researcher, and author in the field of Oral Implantology and Prosthodontics. Dr. Resnik completed his specialty training in Prosthodontics, Fellowship in Oral Implantology, and a Master’s degree in Oral Implantology/Radiology from the University of Pittsburgh School of Dental Medicine. He is the director of the Misch Resnik Implant Institute as well as holds faculty positions at University of Pittsburgh (Graduate Prosthodontics), Temple University School of Dentistry (Graduate Periodontics and Oral Implantology), and Allegheny General Hospital in Pittsburgh, Pennsylvania (Oral and Maxillofacial Surgery). Along with his passion for lecturing and education, Dr. Resnik is also an accomplished author, having published over 100 articles and author of the two leading textbooks in Implant Dentistry: Avoiding Complications in Oral Implantology and the 4th edition of Contemporary Implant Dentistry.
Randolph R. Resnik, DMD, MDS, is a leading clinician, educator, researcher, and author in the field of Oral Implantology and Prosthodontics. Dr. Resnik completed his specialty training in Prosthodontics, Fellowship in Oral Implantology, and a Master’s degree in Oral Implantology/Radiology from the University of Pittsburgh School of Dental Medicine. He is the director of the Misch Resnik Implant Institute as well as holds faculty positions at University of Pittsburgh (Graduate Prosthodontics), Temple University School of Dentistry (Graduate Periodontics and Oral Implantology), and Allegheny General Hospital in Pittsburgh, Pennsylvania (Oral and Maxillofacial Surgery). Along with his passion for lecturing and education, Dr. Resnik is also an accomplished author, having published over 100 articles and author of the two leading textbooks in Implant Dentistry: Avoiding Complications in Oral Implantology and the 4th edition of Contemporary Implant Dentistry.
References
- Abusamaan M, Giannobile WV, Jhawar P, Gunaratnam NT. Swallowed and aspirated dental prostheses and instruments in clinical dental practice. J Am Dent Assoc. 2014;145(5),459-463.
- Wazani EI, Nixon BP, Butterworth CJ. Accidental Ingestion of an Implant Screwdriver: A Case Report and Literature Review. Eur J Prosthodont Restor Dent. 2018; 26(4):18,
- Black RE, Johnson DG, Matlak ME. Bronchoscopic removal of aspirated foreign bodies in children. J Pediatr Surg. 1994;29(5):682-684.
- ASGE Standards of Practice Committee, et al. Management of ingested foreign bodies and food impactions Gastrointest Endosc. 2011;73(6):1085-1091.
- Ireland AJ. Management of inhaled and swallowed foreign bodies. Dent Update. 2005;32:83-86, 89.
Stay Relevant With Implant Practice US
Join our email list for CE courses and webinars, articles and mores

