
Dr. Suheil M. Boutros describes a technique that strives to create ideal esthetics and function
Immediate implant placement has been advocated to minimize hard tissue loss following tooth extraction.
[userloggedin]
On the other hand, immediate provisionalization enables the maintenance of the gingival architect for optimal esthetic emergence profile and eliminates the need for a removable provisional prosthesis while osseointegration is achieved. This case report describes a technique that enables the restorative team to create ideal esthetics and function following immediate placement and provisionalization.
In addition, this case demonstrates the predictable outcome of using short implants in combination with CAD/CAM restorations.
Introduction
Patients with congenitally missing teeth are seeking dental implant therapy more than conventional replacement due to the higher success rate. Generally, these patients have less than ideal alveolar bone width due to the absence of the permanent teeth. In addition, most retained primary teeth in the posterior regions have mucogingival defects. In these situations, incorporating the principles of periodontal plastic surgery along with the concept of immediate non-functional loading allows the development of a healthy and an esthetic emergence profile. Furthermore, with the utilization of the BellaTek® Encode® system, these implants can be restored with custom abutments that will provide the most optimal gingival contours and esthetics.
Patient presentation
This clinical presentation demonstrates the replacement of a congenitally missing maxillary left second premolar. A 40-year-old female presented with a primary retained maxillary left second molar that resulted in severe gingival recession. The patient was also missing the mandibular second premolars, first and second molars bilaterally. The patient did not have a medical or dental contraindication for implant therapy.
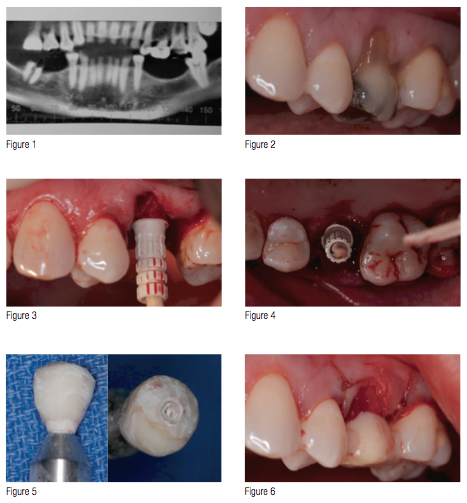
Following the evaluation of the cone beam CT scan (Figure 1), the patient was given the option of extraction of the primary maxillary left second molar and immediate implant placement along with mucogingival surgery to manage the mucogingival defect (Figure 2). Concurrently, the mandibular posterior teeth will be replaced with dental implants.
Surgical treatment
At the surgical appointment, under intravenous conscious sedation using Midazolam (5 mg) and Fentanyl (100 mcg) along with the administration of local anesthesia, the primary retained maxillary left second molar was atraumatically extracted. The osteotomy was prepared in a type II-III bone. Bone taps were not used before the placement of a 4-mm diameter by 13-mm length Biomet 3i™ OSSEOTITE® Tapered Certain® Implant. A PreFormance® Post was used to support a resin-bonded screw-retained restoration (Figures 3-5).
Following the seat of the provisional restoration, the flap was coronally advanced using Ethicon 4-0 Vicryl™ suture without the use of a free connective tissue graft (Figures 6-7).
At the same surgical visit, six 4-mm diameter by 8.5-mm length Biomet 3i OSSEOTITE Certain Tapered Implants were placed in the posterior mandible along with the extraction of tooth No. 32 (Figure 8). The patient was given post-surgical instructions, including the use of 0.12% chlorhexidine gluconate (Peridex™, Proctor & Gamble) 3 times daily and was prescribed 500 mg of amoxicillin (every 6 hours for 7 days).

Prosthetic treatment
Three months following implant placement, the patient was seen for evaluation of osseointegration, healing was uneventful, and soft tissue healing was optimal (Figure 9).
At the same time, the lower implants were uncovered, and Encode 4 x 4 x 5 mm healing abutments were placed (Figure 10).
Two weeks later, the screw-retained restoration was removed by the restoring dentist, and an Encode 4 x 4 x 5 mm healing abutment was placed (Figure 11). A healing abutment level impression was taken using polyvinylsiloxane impression material (Figures 12 and 13).
In the laboratory, an Encode master cast was fabricated, and the casts were mounted in an articulator on Adesso® Magnetic Mounting Plates (Ivoclar Vivadent Inc.). The mounted casts were then sent to the Biomet 3i PSP Department for scanning and milling of Encode abutments (Figure 14). The milled abutments were returned to the laboratory for the fabrications of the final crowns (Figures 15-17).
The screw-retained restoration was removed, and the Encode abutment was placed. The fit and esthetics were verified clinically and radiographically (Figures 18-22). The Gold-Tite® abutment screws were placed and tightened to 20 Ncm with a Biomet 3i Torque Indicating Rachet Wrench (Figure 23). The final crown was cemented with RelyX™ cement (3M™ ESPE™); excess cement was removed (Figure 22). At the same time, the lower Encode abutments were seated and tightened to 20Ncm; the final splinted crowns were cemented in place using the same cement. Oral hygiene instructions were given, and the patient was seen for follow-up visits at 3 and 6 months, respectively.

Follow-up and maintenance

The patient was seen for a follow-up visit at 3 months (Figure 23), and at 6 months post placement; the gingival tissues were healthy, and the esthetic outcome was well maintained (Figures 24-25). Currently, the patient is placed on a 6-month recall to properly maintain the implants and the restorations. At 1-year post restoration, the bone level around all implants is well maintained (Figure 26).
Clinical relevance
With patients’ increasing demand for immediate implant placement and immediate provisionalization, it is possible to create soft tissue symmetry and health around implant-supported crowns through the use of properly shaped provisional restoration, while allowing the patient to function, feel, and look esthetically pleasing during the osseointegration period.
This case also demonstrated that the combination of short implants and the very precise CAD/CAM restoration can achieve a very predictable long-term functional and esthetic outcome.
Stay Relevant With Implant Practice US
Join our email list for CE courses and webinars, articles and mores
