Dr. Paul Stone explains how Straumann’s Roxolid® narrow implant can be placed in more sites and requires less grafting, resulting in greater patient uptake
For many years, the two main dental implant materials available were either grade 4 pure titanium (with very strictly controlled minimal percentages of other elements) or a variety of titanium alloys of which titanium-aluminum-vanadium (TiAl6V4) was the most common.
[userloggedin]
Both performed well enough in the clinical environment, with the grade 4 titanium exhibiting the better biological interaction with the neighboring bone and the titanium alloy having the greater strength.
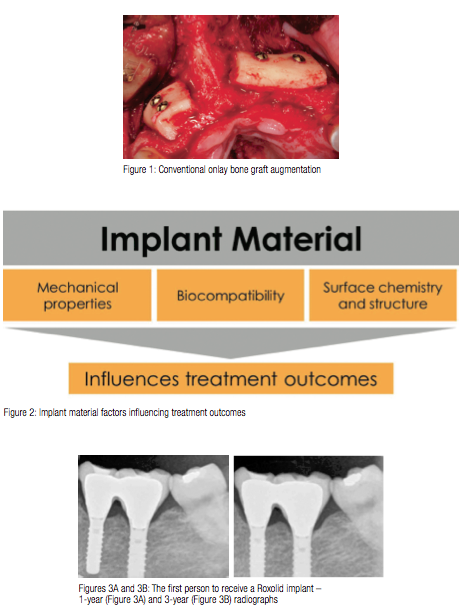
Astime passed, and the expectations of clinicians and patients increased, the boundaries for the existing materials began to be pushed. Implants needed to be placed into narrower spaces, usually due to not only lack of bone width, but also reduced space between teeth (upper laterals, lower incisors, and small premolars). Another factor was to avoid more extensive bone grafting (Figure 1).
While narrow implants were available (usually between 2.5 mm and 3.5 mm diameter), they came with guidelines as to when and how they should be used to reduce overloading issues and were accompanied by publications indicating (not surprisingly) higher fracture rates for the grade 4 titanium designs. There was often a reluctance to use one of the titanium alloys because, although stronger, publications indicated poorer cell integration (inhibition of osteoblast differentiation), and there were concerns that in narrower diameters, the surface area available for cell attachment was even less.
New material
Fortunately, the arrival of a new implant material (the first that was developed exclusively for dental implants) has begun to change some of our previously held concepts. The Swiss dental implant company Straumann has been at the forefront of dental implants from the very beginning, and they looked at evidence from papers published over the last 15 years to develop an alloy of titanium (85%)
and zirconium (15%) that is called Roxolid®. This new alloy also allows for preparation of the implant using the well-evidenced SLActive® surface technology, providing optimal surface texture and hydrophilicity with the highest rates of bone attachment (Figure 2).
Blackhills Clinic was fortunate to have carried out the first-ever treatment in a human using this new implant as part of a pilot study. Our 3-year published results have confirmed that the “test” implants were stable and functional, and demonstrated good osseointegration and no mechanical failure (Figures 3A and 3B). The mean bone change in functional bone level over the 3 years was only 0.3 mm. All surviving implants and restorations were considered to be successful. Since this initial study, many more researchers have looked into this new material, and there is now increasing evidence that the material is not only stronger than grade 4 titanium (by up to 55% and similar to TiAl6V4 alloy), but also exhibits better bone attachment at a cellular level. This means that for the first time, clinicians can have confidence in using reduced diameter implants, both mechanically and biologically.

Careful consideration
At Blackhills Clinic, we now have more than 5 years of experience with reduced diameter Roxolid implants and are in a position to comment on our findings and the implications. It is fair to say that previously, narrower implants were placed with some degree of skepticism, and patients were always warned of the increased risk of mechanical failure. This affected confidence could limit the number of treatment options available, often resulting in more bone graft augmentation to create adequate bone for the wider, stronger implants. With Roxolid, we can confidently explain to patients the nature of the new material and now find that bone grafting is required less frequently. Even where it is necessary, this is now often a straightforward, simultaneous procedure with significantly reduced morbidity, healing time, and cost to the patient. As well as the need for less grafting, the narrower diameter also ensures that there is relatively more bone thickness surrounding the implant that, in turn, results in better long-term stability for both the bone and the overlying mucosa. A more predictable long-term esthetic result is one of the most desirable benefits from using Roxolid implants.
Despite all the advantages of Roxolid, there needs to be some caution when using any reduced-diameter implant. The narrow size necessitates additional restorative considerations regarding the maintenance and appearance of the final restoration. A considerable over-contour or overhang can
result from the abrupt change in diameter from the narrow implant head to the final restoration diameter (Figures 4A and 4B). This can adversely affect the final appearance, especially if the lip line is high or the oral mucosa is particularly thin, creating an unsightly shadow that can then look even worse if there is subsequent shrinkage of the labial soft tissues. The over-contouring can also cause problems with oral hygiene measures and with accurate peri-implant clinical probing assessments, preventing cleaning aids and metal periodontal probes from adapting to the sub-mucosal concavity. It is therefore important that careful consideration is given to the design, manufacture, and maintenance by all involved, and this includes the technician and patient (Figures 5A and 5B).

In summary, Roxolid dental implants show better bone attachment than has been observed with grade 4 titanium or other alloys. Its increased strength means that there are more options for using this narrower implant in more sites and with the need for less grafting (Figure 6). Inevitably this results in a higher patient acceptance. The reduced diameter allows for more favorable bone thickness around the implant than an equivalent regular diameter implant that, in turn, gives better long-term, more predictable support for the overlying soft tissues. On the downside, the reduceddiameter (rather than a particular material) means that care is needed when planning the use of any narrow implant, particularly with a more borderline case or where higher esthetic expectations are involved.
Stay Relevant With Implant Practice US
Join our email list for CE courses and webinars, articles and mores
