Dr. Bart Silverman treats a patient who has cystic fibrosis with platelet-rich fibrin to help with bone regeneration during the implant process.
Dr. Bart Silverman discusses a technique to promote osseointegration for patients with a respiratory disease
Cystic fibrosis is a rare monogenic autosomal recessive genetic disease affecting around 75,000 people worldwide.1 The disease is typically diagnosed at birth and impacts Caucasians of northern European ancestry with an occurrence of 1 in 2,000-3,000 births, and occurs least often in Asian Americans with approximately 1 in 30,000 births.2 It is caused by passing a mutated gene for the cystic fibrosis transmembrane conductance regulator (CFTR) from both parents. The disease process is usually associated with respiratory failure. Patients typically have a life expectancy of approximately 2-30 years.3
Over the past few decades, with advances in pharmacological therapy, patients with cystic fibrosis have been living longer. With an increase in longevity, new long-term complications have arisen. This genetic disorder has been found to affect the pancreas, liver, kidneys, intestine, and bone. Osteopenia (low bone density) is present in up to 50% of all post-pubescent patients. Osteoporosis, a more significant form of bone weakening, is found in 10%-34% of all adult patients presenting with this disease.4 Cystic fibrosis has also been associated with limited Vitamin D absorption.5 A deficiency in vitamin D absorption has been correlated with low bone density and poor bone healing.6 Low vitamin D levels have been correlated with an increased failure rate of bone grafts.7 The low vitamin D level and concomitant osteopenia/osteoporosis can make dental implant placement in areas of potential low bone density challenging in patients with cystic fibrosis.
Platelet rich fibrin is an autologous blood platelet-rich concentrate which has been shown to increase soft and hard tissue healing. It concentrates the patient’s platelets, fibrin, and growth factors.8 Platelets contain α-granules. The α-granules, in turn, contain growth factors that play a significant role in tissue healing. When platelets become activated and degranulate, the growth factors contained within the α-granules are released.9 The released growth factors provide parenchymal signaling for the recruitment of cytokines and stem cells into the surgical area.10 These stem cells differentiate into soft tissue and bone-forming cells. These recruited cells further bone regeneration.12 The placement of autogenous platelet concentrates in surgical areas has been shown to increase the rate of bone formation, bone density,13 and quality of the healed bone.14 Platelet concentration techniques may be used in compromised situations to aid in healing and possibly prepare an osseous site for future dental implant placement(s).

Clinical case report
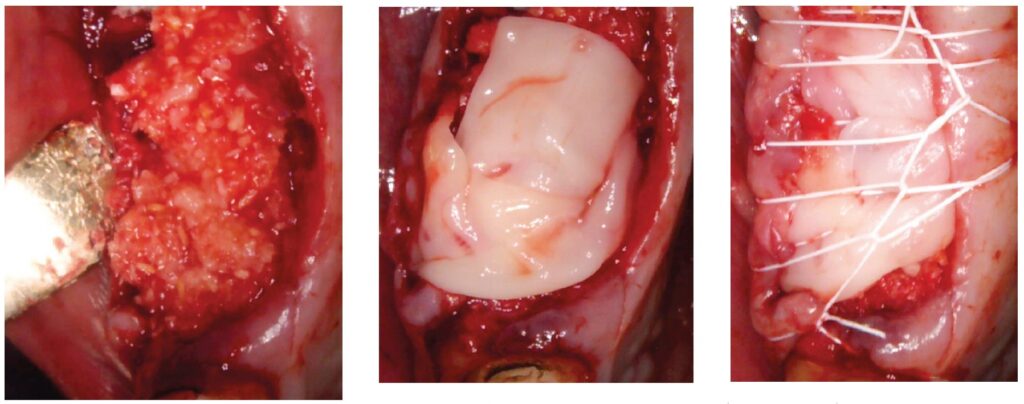
A 64-year-old male presented to the dental clinic for extraction of non-restorable maxillary left first, second, and third molars in January 2019. The past medical history was significant for cystic fibrosis and depression. He had an allergy to sulfa medications and was taking the following medications: Pulmozyme® (dornase alpha), testosterone, prednisone, and nifedipine. The patient presented with a chief complaint of “I didn’t think I was going to live this long with cystic fibrosis, but I did, and now I am ready to take care of my needs.” The clinical examination was significant for a grossly carious dentition in need of repair (Figure 1). After reviewing several options, it was decided to extract the non-restorable left maxillary first, second, and third molars and to restore the maxillary left first and second molars with fixed implant-retained restorations. With potential healing concerns secondary to his cystic fibrosis, the addition of platelet-rich fibrin (PRF) was discussed. The patient was taken to the surgical operatory where the blood pressure was taken, a pulse oximeter placed, and an IV was started using a 21-gauge butterfly catheter in the right antecubital fossa. PRF protocol was followed using Intraspin® centrifuge (BioHorizons; Birmingham, Alabama), and anesthesia was maintained thereafter using a balance technique. Maxillary left first, second, and third molars were surgically removed, and the resulting extraction sockets were curetted free of granulation tissue. PRF clots and membranes were prepared as described by Choukroun, et al.15 The PRF was mixed 50/50 with MinerOss® mineralized allograft cancellous bone particles (BioHorizons; Birmingham, Alabama) resulting in a “sticky bone preparation” that was placed in the maxillary left first and second molar sockets (Figure 2). Two PRF membranes were placed across the extraction sites (Figure 3), and 3-0 PTFE interrupted sutures were placed affording good wound apposition (Figure 4). Adequate soft tissue healing was observed at a 3-week postoperative check.
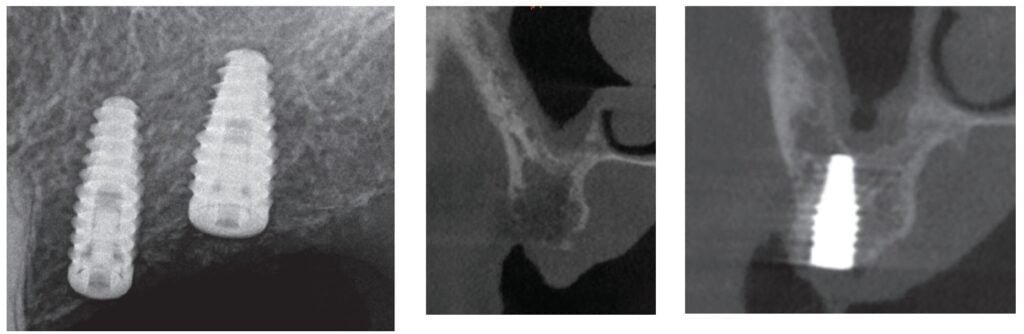
The patient returned a year later in December 2019 after receiving bilateral knee replacements. He wanted to fully recover and rehab from the knee reconstructive surgery before having his dental implants placed. A panoramic radiograph and CBCT were performed with Carestream CS9300 (Carestream Atlanta, Georgia) (Figures 5 and 6). The patient was taken to the oral surgical suite where a 23-gauge butterfly intravenous catheter was started in the right antecubital fossa, and anesthesia was maintained thereafter with a balance technique. A crestal incision was performed, and a full-thickness flap was reflected. Osteotomies were performed using appropriate drills. A BioHorizons Tapered Pro 4.2 mm x 12 mm implant was placed at tooth No. 14 position, and a BioHorizons Tapered Pro 5.2 mm x 10.5 mm implant was placed at tooth No. 15 area. Both implants were placed with greater than 35 ncm torque values (Figure 7). Gingival former healing collars were placed for single stage implant surgery. The wound was closed using interrupted sutures, and the patient was discharged in the care of a family member.

implant placement

One can appreciate the decrease in bone density in the ungrafted posterior maxilla (Figure 8) and the moderately more dense appearance in the grafted site where the PRF graft changed the local topography (Figure 9). The implants have subsequently integrated, and the patient is waiting to return to the restorative dentist when “he feels comfortable returning to a dentist office post-COVID” for a planned splinted cement-retained restoration. In the posterior maxillary region, this restoration would allow a greater chance of success in the D3 bone.
Discussion
The life span of patients with cystic fibrosis has increased, and there is a tendency to see complications with organ systems other than just pulmonary. Problems with bone metabolism have been noted. With patients presenting for dental implants, clinicians must do what they can to increase the potential for osseointegration and successful outcomes. Autologous growth factors have been shown to improve bone healing.8,11,12 This case demonstrates the use of PRF in a medically compromised patient, one with cystic fibrosis, to change the bony landscape and provide a more predictable and enhanced outcome. This is one case supporting this theory, and more work needs to be performed in the future with these clinical situations.
Read more about how platelet-rich fibrin can help promote tissue healing and regeneration. https://implantpracticeus.com/ce-articles/a-comprehensive-clinical-review-of-platelet-rich-fibrin-and-its-role-in-promoting-tissue-healing-and-regeneration-part-1/
 Bart Silverman, DMD, graduated from Fairleigh Dickinson University in 1982 Summa Cum Laude and received his Doctorate in Dental Medicine in 1986 from Fairleigh Dickinson Jr. School of Dentistry, where he was a member of the Omicron Kappa Upsilon Honor Society. He completed his Oral and Maxillofacial residency at Westchester County Medical Center in 1989 and was chief resident in his final year. He is in private practice limited to Oral and Maxillofacial Surgery in New City, New York and is a Diplomate of the American Board of Oral and Maxillofacial Surgery and the American Board of Oral Implantology. He has been lecturing in the field of implant dentistry for over 25 years. Dr. Silverman is an Attending Physician at Westchester County Medical Center, Department of Oral and Maxillofacial Surgery, a Clinical Associate Professor at New York Medical College, Adjunct Clinical Associate Professor Department of Oral and Maxillofacial Surgery at New York University School of Dentistry, and Surgical Director of NYU Post-graduate Continuing Education Dental Implant Program. He is also an Adjunct Clinical Associate Professor at Roseman School of Dentistry, Director of Roseman University Maxicourse in Implant Dentistry, Director BWS Dental Seminars, Faculty at Implant Pathways, and New York, Chicago, and Rutgers, Asia Dental Implant Maxicourses.
Bart Silverman, DMD, graduated from Fairleigh Dickinson University in 1982 Summa Cum Laude and received his Doctorate in Dental Medicine in 1986 from Fairleigh Dickinson Jr. School of Dentistry, where he was a member of the Omicron Kappa Upsilon Honor Society. He completed his Oral and Maxillofacial residency at Westchester County Medical Center in 1989 and was chief resident in his final year. He is in private practice limited to Oral and Maxillofacial Surgery in New City, New York and is a Diplomate of the American Board of Oral and Maxillofacial Surgery and the American Board of Oral Implantology. He has been lecturing in the field of implant dentistry for over 25 years. Dr. Silverman is an Attending Physician at Westchester County Medical Center, Department of Oral and Maxillofacial Surgery, a Clinical Associate Professor at New York Medical College, Adjunct Clinical Associate Professor Department of Oral and Maxillofacial Surgery at New York University School of Dentistry, and Surgical Director of NYU Post-graduate Continuing Education Dental Implant Program. He is also an Adjunct Clinical Associate Professor at Roseman School of Dentistry, Director of Roseman University Maxicourse in Implant Dentistry, Director BWS Dental Seminars, Faculty at Implant Pathways, and New York, Chicago, and Rutgers, Asia Dental Implant Maxicourses.
- Fajac I, Wainwright C. New treatments targeting the basic defects in cystic fibrosis. Presse Med. 2017 Jun;46 (6 Pt 2): e165-e175. Epub.
- Rafeeq MM, Murad HAS. Cystic fibrosis: current therapeutic targets and future approaches. J Transl Med. 2017;15(1):84.
- Putman MS, Anabtawi A, Le T, Tangpricha V, Sermet-Gaudelus I. Cystic fibrosis bone disease treatment: current knowledge and future directions. J Cyst Fibros. 2019 Oct; 18 Suppl 2:S56-S65.
- Chedevergne F, Sermet-Gaudelus I. Prevention of osteoporosis in cystic fibrosis. Curr Opin Pulm Med. 2019 Nov;25(6):660-665.
- Hall WB, Sparks AA, Aris RM. Vitamin D deficiency in cystic fibrosis. Int J Endocrinol. 2010;2010:218691. Epub 2010 Jan 28.
- Reid IR. Vitamin D effect on bone mineral density and fractures. Endocrinol Metab Clin North Am. 2017;46(4):935-945.
- Choukroun J, Khoury G, Khoury F, Russe P, Testori T, Komiyama Y, Sammartino G, Palacci P, Tunali M, Choukroun E. Two neglected biologic risk factors in bone grafting and implantology: high low-density lipoprotein cholesterol and low serum vitamin D. J Oral Implantol. 2014 Feb;40(1):110-114.
- Miron RJ, Zucchelli G, Pikos MA, Salama M, Lee S, Guillemette V, Fujioka-Kobayashi M, Bishara M, Zhang Y, Wang HL, Chandad F, Nacopoulos C, Simonpieri A, Aalam AA, Felice P, Sammartino G, Ghanaati S, Hernandez MA, Choukroun J. Use of platelet-rich fibrin in regenerative dentistry: a systematic review. Clin Oral Investig. 2017 Jul;21(6):1913-1927.
- Marx RE. Platelet-rich plasma: evidence to support its use. J Oral Maxillofac Surg. 2004;62(4):489-496.
- Kang YH, Jeon SH, Park JY, Chung JH, Choung YH, Choung HW, Kim ES, Choung PH. Platelet-rich fibrin is a Bioscaffold and reservoir of growth factors for tissue regeneration. Tissue Eng Part A. 2011 Feb;17(3-4):349-59.
- Srinivas B, Das P, Rana MM, Qureshi AQ, Vaidya KC, Ahmed Raziuddin SJ. Wound healing and bone regeneration in postextraction sockets with and without Platelet-rich Fibrin. Ann Maxillofac Surg. 2018 Jan-Jun;8(1):28-34.
- Zhang Y, Ruan Z, Shen M, Tan L, Huang W, Wang L, Huang Y. Clinical effect of platelet-rich fibrin on the preservation of the alveolar ridge following tooth extraction. Exp Ther Med. 2018 Mar;15(3):2277-2286.
- Marx RE, Marx RE, Carlson ER, Eichstaedt RM, Schimmele SR, Strauss JE, Georgeff KR. Platelet-rich plasma: Growth factor enhancement for bone grafts. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998 Jun;85(6):638-46.
- Kang YH, Kang YH, Jeon SH, Park JY, Chung JH, Choung YH, Choung HW, Kim ES, Choung PH. Platelet-rich fibrin is a bioscaffold and reservoir of growth factors for tissue regeneration. Tissue Eng Part A. 2011 Feb;17(3-4):349-59.
- Choukroun J, Adda F, Schoeffler C, Vervelle A. An opportunity in perio-implantology: The PRF. 2001;42:55-62.
Stay Relevant With Implant Practice US
Join our email list for CE courses and webinars, articles and mores

