Dr. David Speechley delves into the surprising history behind bisphosphonates and the terrible legacy of “phossy jaw”
The year was 1669 when German scientist Hennig Brand first discovered the philosopher’s stone — or so he thought. His experiment had started with ingredients that included sand and more than 50 buckets of urine, and the process had taken 2 weeks to complete; but the product of his labor was a substance that glowed in the dark.
 Nothing like this had ever been seen before, so he really did believe he had discovered something with magic properties. Calling his discovery phosphorus (meaning “bringer of light” in Greek), scientists all over Europe were soon engaged in trying to unlock the magic properties of this wondrous substance, with eminent people such as Robert Boyle giving demonstrations in the United Kingdom to his fellow scientists.
Nothing like this had ever been seen before, so he really did believe he had discovered something with magic properties. Calling his discovery phosphorus (meaning “bringer of light” in Greek), scientists all over Europe were soon engaged in trying to unlock the magic properties of this wondrous substance, with eminent people such as Robert Boyle giving demonstrations in the United Kingdom to his fellow scientists.
Today, we know that phosphorus is a non-metallic element, essential for life that is present in bone as well as both DNA and RNA. Its modern uses include pesticides, pyrotechnics, steel production, armaments, and pharmaceuticals; but back in the 17th century, its practical use was limited.
A darker side
In 1831, the Frenchman Charles Sauria invented a “strike-anywhere” match, the head of which contained a mixture of white phosphorus, potassium chlorate, gum, and starch. These matches ignited when rubbed on a rough surface, and the match industry was born.
Founded in 1850, the Bryant and May match company rose in importance and, by 1861, had become one of England’s largest employers, operating from the largest industrial complex in Britain, situated in the Bow area of London. The workforce ran into the thousands and was largely made up of women, mostly young.
Conditions were atrocious with work-related deaths commonplace. The workers suffered from abdominal pain, liver and kidney damage, central nervous system disturbances, and phossy jaw.
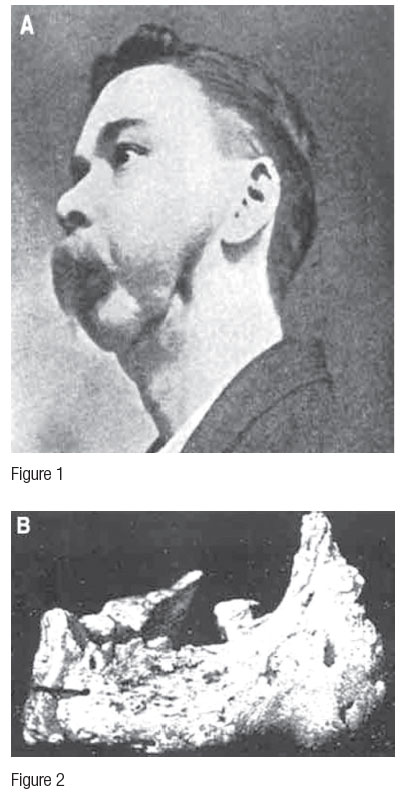
Phossy jaw was a dreadful condition typified by necrosis of the jawbones, eroding away the lower face, leading to an agonizing death. Many young workers imbibed such quantities of phosphorus from the working environment that reportedly girls as young as 13 in the cold winter nights had mandibles that could be clearly seen glowing through their skin. Figure 1 is an image from the mid-1850s, of a man suffering from phossy jaw. Figure 2 is his mandible postmortem.
Yesterday’s poison
By 1888, the workforce was so dis-contented that they marched on Parliament. Nearly 1,500 workers withdrew their labor, and Bryant and May was forced to take note.
Dentists employed to research the condition of phossy jaw concluded that the condition was brought about by phosphorus poisoning, and that the severity of the condition was related to how closely the workers worked to the cauldrons containing the noxious chemicals and over what time scale. The dentists concluded that the symptoms were time- and dose-related.
Today, we know the mechanism of the condition; the white phosphorus was reacting with water, carbon dioxide, and amino acids within the bodies of the workers to produce amino bisphosphonate. These poor unfortunates were imbibing un-controlled doses of bisphosphonates and suffering bisphosphonate-related osteo-necrosis (BRON — though there are a number of acronyms for this condition).
Bisphosphonate-related osteonecrosis of the jaw is today defined as:
- Current or previous treatment with bisphosphonates
- Exposed bone in the maxillofacial region persisting for more than 8 weeks
- No history of radiotherapy to the jaws (American Association of Oral and Maxillofacial Surgeons, 2006)
The poisonous effects of bisphosphonates were clearly now well established — but as history has shown time and again, yesterday’s poison is tomorrow’s wonder drug, and bisphosphonates have been no exception.
Today’s wonder drug
Today, bisphosphonates are a class of drugs that prevent the loss of bone mass.They are used to treat metabolic disorders of bone, including Paget’s disease, osteoporosis, osteogenesis imperfecta, and more life-threatening conditions such as multiple myeloma, primary bone malignancies, and metastases from other malignancies, including breast and prostate.
Their mode of activity is preventing bone remodeling: The bisphosphonate molecule enters the osteoclast cell and brings about apoptosis. The dead cell gives up its contents, including the unchanged bisphosphonate molecule, which can go on to enter another cell. The half-life of this drug is therefore long, with authors recording figures of around 10 years.
Applications
Bisphosphonates are the only drugs effective in prolonging life of those suffering from hypercalcaemia of malignancy, although this remains a terminal condition, and their life-extending properties are limited.
Osteitis deformans (Paget’s disease of bone) is a relatively common condition in which the cycle of bone turnover is disrupted. This can cause bones to become weakened and deformed, and results in symptoms that may include pain and deformity. It is the second most common metabolic disorder of bone after osteoporosis.
The condition shows familial tendencies and is most widespread in the U.K. (the north west in particular), but it occurs in countries that have experienced migration from the U.K. as well – most notably the United States, Australia, New Zealand, and South Africa.
The onset of Paget’s disease is age-related; 1%-2% of white adults who are over 55 years of age have Paget’s disease, rising to 5%-8% for white people who are over the age of 80. The causes of Paget’s disease are not fully established, but it seems that two rogue genes are implicated and a viral trigger, which may be the measles virus. One theory is the mutated genes RANKL and SQSTM1 cause the measles virus to remain in the body following infection, lying dormant for decades before being reactivated and attacking the osteoclast cells, causing them to malfunction. The decline in the incidence of both measles and Paget’s disease could therefore be related.
Until the 1960s, treatment of Paget’s disease was limited to hormonal treatment and surgery to correct bony deformities, including the removal of lumps and bumps impinging on nerves causing neurological disturbances. It is said the sciatic nerve, with its long tortuous path, is particularly vulnerable, and people suffering repeated bouts of sciatica should be tested for Paget’s. Serum alkaline phosphatase (SAP) remains the definitive blood test, and diagnosis may happen when a person is having a blood test for another unrelated condition, since most sufferers have little or no symptoms.
Today, bisphosphonates taken either orally or by infusion are the drugs of choice in the treatment of people experiencing the bony symptoms of Paget’s disease. These drugs work by suppressing the actions of the osteoclasts — since osteoclastic activity triggers osteoblastic activity, the bone remodeling process is inhibited and bone density maintained. The dosage typically used makes it likely that these people may well be suitable for implant placement, but liaison with the clinician treating the condition should be consulted prior to considering dental implantation.
Taking bisphosphonates
Oral bisphosphonates should be taken on an empty stomach to aid absorption. They should be taken while standing, or sitting upright, and taken with water, refraining from food for approximately 2 hours.
Common side effects include diarrhea and nausea. More rarely, side effects may include a tingling sensation in the arms or legs, as well as changes in mental states (such as confusion), hair loss, headaches, and glossitis. In recent times following the trend in the U.S., the oral route is becoming less popular, giving way to infusions.
Osteoporosis
In the last 15 years or so, bisphosphonates have become the drugs of choice for the treatment of osteoporosis, a condition in which the bone mineral density is reduced beyond certain limits, the diagnosis being made by dual energy X-ray absorptiometry (DEXA) scanning.
We must consider when the loss of bone mineral density — something that occurs with increasing age in both sexes, but most notably in post-menopausal women — ceases to be physiological and becomes pathological, and also what the consequences of not treating this condition may be.
DEXA scans measure bone mineral density and are reported as T-scores, comparing the patients’ bone mineral density with the optimal peak mineral density for their gender, or as Z-scores when comparison is drawn with individuals of the same age, weight, ethnicity, and gender. The latter may be more useful as it allows for changes, which are known to occur with aging.
Osteoporotic fracture is common, expensive, and associated with increased morbidity and mortality. The incidence of osteoporosis-related fracture reported annually in the U.S. is greater than the risk of stroke, breast cancer, and heart attack combined. Statistical analysis reveals that approximately one in two women and one in four men over the age of 50 will suffer osteoporosis-related fractures in their remaining lifetime. In 2005, osteoporosis was responsible for more than 2 million fractures in the U.S., with up to 38% of people who suffered hip fracture attributed to osteoporosis dying within 12 months.
These figures are compelling evidence for why we should be treating osteoporosis.
When it comes to the treatment of malignant bone disease, be it primary bone malignancy or metastatic spread, bisphosphonates are effective in reducing the risk of pathological fracture and confining tumor cells.
The dosage used in these patients tends to be elevated in both dose and potency when compared with the treatment of other conditions, and the effect in the mouth where bone turnover is rapid may be profound.
Stay Relevant With Implant Practice US
Join our email list for CE courses and webinars, articles and mores

