Dr. Andy Denny and Mr. Mike Fuse illustrate a case involving immediate-loaded fixed-implant bridge reconstruction
The All-on-4® treatment concept was developed in the 1990s as a way to best restore the full arches of the upper and lower jaws. The procedure uses only four implants to secure all teeth in place, hence the name “All-on-4.”
[userloggedin]
The All-on-4 treatment concept, using biomechanics, computer simulation, and clinical research, was developed by implant manufacturer Nobel Biocare® and European implant dentist Dr. Paulo Malo. Their results provided patients with high-quality, full-arch restoration for edentulous, compromised-bone patients without the use of bone grafting in the shortest time possible.
For candidates eligible for the All-on-4 treatment concept, the general process for treatment involves just two stages: consultation/assessment and surgery. During the consultation, the candidate undergoes an assessment where eligibility is determined, dental needs are assessed, and a solution is prescribed. The next step in the consultation process is 3D CT scanning where state-of-the-art technology is employed to plan the surgery. The final step in the consultation process is taking impressions so a prosthetic setup can be created to produce the teeth that will be fitted the day of the surgery. Following the consultation stage, the next stage is surgery during which the implants are placed into the patient’s mandible, and/or maxilla, and new teeth are fitted to the dental implants. Four implants can be used to support a fixed prosthesis with 12 to 14 teeth that is placed immediately on the day of surgery.
Case presentation
Assessment and pre-surgical work-up
The patient attended the practice for an initial consultation to find out what his options were to replace his old full upper and lower dentures. His dentures were loose, ill-fitting, and uncomfortable, and he specifically wanted to investigate implant treatment options, having read an article about the All-on-4 treatment concept in the press.
Options:
- Dental implant-supported denture on multiple fixtures with custom-milled retaining bar.
- Dental implant-retained denture on fixtures with locator attachments.
- 6–10 dental implants with multiple short-span ceramic bridges and crowns (potentially involving hard and soft tissue grafting/augmentation).
- All-on-4 treatment concept.
From the options presented, the patient chose the All-on-4 treatment concept as it offered the best fixed solution to meet his needs, and his clinical and radiographic assessment indicated that it was possible.
As the patient’s old dentures were inadequate, impressions and records for new mock-up teeth were set up to try-in, and were approved by the patient. The new acrylic dentures were then created ready for the surgical appointment and duplicated to make acrylic radiographic guides with 8–10 radiopaque markers in.
A dual arch CBCT scan was performed on a J. Morita Veraviewepocs 3D R100 using 80 x 80 FOV. Individual scans were taken of the guides too. All data were imported in to Nobel Biocare’s NobelClinician™ software, and the images married together to show detailed relationship between guides and patient scan.
The digital imaging was evaluated, and a detailed plan formulated in conjunction with technician Mike Fuse of Fusion Dental Ceramics. This plan included the positioning for best anterior-posterior spread and distribution of forces using angled distal fixtures (as per the treatment protocol), and the type of implants identified along with abutment selection to give optimum prosthetic screw access.
Once approved, the plan was digitally sent to Nobel Biocare for production of upper- and lower-guided surgery drill positioning guides.
Surgery and immediate bridge fit
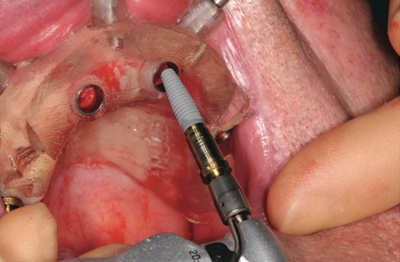
Following local anesthetic, the drill guides were secured in place with guide pins laterally into the ridges, and four NobelReplace™ Tapered Groovy implants were placed in each jaw, using the guided surgery kit, allowing for accurate fixture placement to the pre-assigned depth and position as planned using a flapless surgical technique.
The lower jaw was done first in order that the patient’s bite could be registered against the new upper denture, followed by the upper arch surgery. The distal implants were placed at approximately a 30o angle to achieve maximum advantage to the existing bone structure. Once the four implants were secured, the guides were removed, and 30º angled abutments were attached to the distal fixtures.
Multi-unit screw-retained impression copings were used for open-tray pickup. The copings were linked using LuxaBite® (DMG), and Honigum® heavy automix putty (DMG) was used for the impression, allowing the technician to cast up implant replica models.
The lower denture position was registered over locating copings on the fixtures with O-Bite™ (DMG) and against the upper denture in centric occlusion.
Lab procedure
Before beginning an All-on-4 treatment concept full dual-arch rehabilitation case, it is important to establish a solid occlusion for working on one arch — you can’t just guess where teeth are going to go.
As this was a guided case, it was possible to make the lower provisional from the guided model before the surgery was carried out. The two anterior fixtures were attached so the prosthesis was partially completed and ready to be screwed onto the implants on the day of surgery.
Once the lower prosthesis was screwed in, this gave a solid occlusion to work with when placing the upper arch. As previously described, custom-made transfer copings were used as a reference when registering the upper-arch relationship. These copings were screwed on top of the implant fixture/abutments, and an impression/registration taken inside the denture. The copings were then removed from the patient’s mouth and screwed back into the model to create an accurate reference for adjusting the upper arch.
This compares very favorably with the more common approach that involves cutting large access holes in the denture and filling it up inside the patient’s mouth with cold-cure acrylic. The approach used in this case is far less messy, and far more accurate. The main work is done lab-side while the patient is having a rest from the treatment.
Finishing stages
While the lab process was being completed, the patient was able to have a light lunch and read while awaiting delivery of his provisional fixed bridges.
After a couple of hours, the finished upper- and lower-arch provisional bridges were ready. They were tried in, the esthetics, phonetics, and occlusion checked, and the abutment screws torqued down to 15 Ncm. The access holes were filled with PTFE and Cavit™ (3M™ ESPE™) temporary filling material.
The patient was delighted with the result and the efficiency of the whole process. At the 1-week review, the patient reported little postoperative discomfort: He was able to eat comfortably once more, his speech was normal, and he was amazed with the result.
Because only four implants are used in the procedure, and no extended surgical flaps need to be raised, the entire process is much less invasive and involves less surgical time than other full arch treatment modalities.
The beauty of this procedure is the sheer convenience. The implants developed for this treatment allow for the immediate fitting of replacement teeth to the abutments. This means that with only four implants, patients can leave the practice with a full set of new replacement teeth (in most cases) with no bone grafts necessary. The teeth are fixed, so there is no need for patients to be without teeth or to endure temporary dentures for an extended time period. The patient is enabled to come for a morning appointment and leave that same afternoon with a brand-new smile!
Occasional review appointments take place over the course of the following weeks and months to ensure that that the soft tissues have properly healed and that the implants have successfully integrated. Following this, the patient is required to schedule the final visits for construction of the definitive long-term titanium-reinforced bridge and to arrange regular hygienist appointments for routine maintenance.
The result is a brand-new long-lasting smile with maximum comfort, support, and functionality. Most importantly, patients will walk out of the practice with a boost of self-confidence and an irresistible urge to smile more often, losing any previous feelings of discomfort or self-awareness.
Stay Relevant With Implant Practice US
Join our email list for CE courses and webinars, articles and mores
