Drs. Mathieu Goudal and Cécile Bailly offer a closer look at managing atrophic posterior mandibular regions with The CAD/CAM SUB Implant™ by Panthera Dental.
Drs. Mathieu Goudal and Cécile Bailly discuss a solution for managing atrophic posterior mandibular regions
To this day, the dental implant rehabilitation of atrophic mandibular lateral regions remains a biological, temporal, and financial challenge. Thanks to CAD/CAM, titanium subperiosteal implants have become a viable alternative to conventional axial implants and bone regeneration.
Summary
Subperiosteal implants have a bad reputation due to outdated practices. The main drawbacks — lack of adjustment and biocompatibility — were corrected using CAD/CAM and titanium. New products have entered the market over the past few years. The CAD/CAM SUB Implant™ by Panthera Dental, developed in collaboration with Dr. Yvan Poitras, offers a solution in managing atrophic posterior mandibular regions.
History
First described by Dr. Gustav Dahl in 1940, subperiosteal implants allowed for fixed denture rehabilitation for complete or posterior edentulism (Class I).1 These implants were custom-made cobalt-chrome subperiosteal frames with transmucosal abutments to anchor implant-supported dentures. Made-to-measure implants were created using a direct bone impression after elevating large, full-thickness flaps. The frame was placed on the residual bone and stabilized using retaining screws, while possible adjustment defects were corrected through drilling or filling the space with bone substitute.2
Subperiosteal implants had a survival rate of 50% to 60% after 15 years with significant complication risks.3 The lack of osseointegration and the poor precision of the impression caused a lack of stability and adaptation of the metal frame and led to infection, inflammation, and bone resorption.4,5 These implants gradually became less popular and were replaced by endosseous implants, which were more reliable in the short and long term.6
Physiopathology of the mandible
However, in severe cases of atrophy, denture rehabilitation using axial implants can be very complex due to the loss of the alveolar bone. The alveolar bone exists solely for the dental organ, which is where this bone develops and grows. Teeth, the periodontal ligament, and the alveolar bone are therefore interdependent.
After edentulism, the labial alveolar bone will gradually decrease in height, density, and thickness. The loss of function of the alveolar bone and the stress it undergoes will cause resorption that begins in the periosteum, and bone apposition may decrease or even cease.7,8 If edentulism is not compensated, the alveolar bone will continue to undergo resorption and may even be lost completely. In the most serious cases of mandibular atrophy, basal bone loss can occur.
Conversely, an alveolar osteolysis caused by periodontitis leads to dental organ loss. Some bacteria involved in periodontal disease associated with unfavorable local and immune factors cause alveolar bone loss that leads to edentulism.9 In advanced stages, periodontitis can cause complete alveolar bone loss, even after edentulism.
This bone loss intensifies with age. The expression of homeogenes and hormones responsible for alveolar bone maintenance decreases with age, causing decalcification and bone destruction. Denture rehabilitation may be iatrogenic for the remaining bone, and wearing unstable and poorly adapted removable dentures may overload the alveolar bone, causing resorption as a defense mechanism. A failed implant rehabilitation may also increase the loss of residual bone volume.
Alveolar bone loss follows a predictable pattern represented by the Cawood physiopathological classification. This classification allows clinicians to choose the denture rehabilitation approach best suited to each situation.10 The edentulous mandible undergoes significant resorption and loses 40% to 60% of its height on average. At atrophic stages, the mandibular canal may be level with the alveolar ridge, compromising denture rehabilitation.11
Placing axial implants in severe cases of atrophy may require rearranging bone mass through guided bone regeneration, distraction osteogenesis, or crestal reconstruction through bone grafting.12-14 With these implant surgeries in atrophic areas, there are risks of hemorrhage and lesions to neighboring anatomical and nervous structures.
The results of mandibular bone volume reconstruction are fairly unpredictable, as the spongy bone is dense and the cortical bone is thick, thereby reducing blood flow and regenerative potential. It is a long, expensive technique that requires two surgeries with significant healing periods: one for crestal reconstruction and another for implant placement. Success depends heavily on the surgeon’s experience with the procedure.
For the rehabilitation of atrophic posterior mandibular regions, subperiosteal implants are an alternative worth exploring. Placing this implant is technically simpler for the surgeon and can be done in a single procedure with a shorter healing period.
Anatomy review and surgical approach
The mandible is characterized by the presence of the mandibular canal containing the inferior alveolar nerve, along with venous, arteries, and lymphatic vessels. This canal enters the mandible at its ramus through the mandibular foramen, runs through the body of the mandible, and exits through the mental foramen. The inferior alveolar nerve is the motor for the anterior belly of the digastric and the mylohyoid muscles. It also supplies sensation for mandibular teeth, the lower lip, and the chin. The pathway of the mandibular canal is variable and must undergo preoperative examination by analyzing a CBCT.
The lateral aspect of the posterior region of the mandible presents the external oblique ridge and is the insertion for the cutaneous muscles of the cheek. Its medial aspect is connected to the floor of the mouth formed by the mylohyoid and geniohyoid muscles, as well as the tongue. It presents the internal oblique ridge, the insertion point for the superior pharyngeal constrictor, the pterygomandibular ligament, and the mylohyoid muscle in continuity with the periosteum.
This area is adjacent to the submandibular and sublingual spaces, which are rich in neurovascular structures.
The submandibular space is characterized by the presence of the submandibular salivary gland, the hypoglossal nerve (XII, motor nerve of the tongue), the lingual nerve, the facial and lingual artery, and the facial and superior thyroid veins. The sublingual space, located between the floor of the mouth and the mylohyoid muscle, contains the sublingual salivary gland, the deep-lingual vein, the hypoglossal nerve (taste and tongue sensation, visceral motor of the salivary glands), and the submandibular duct15 (Figure 1).
Surgery in the posterior region of the mandible is delicate due to the proximity of the sublingual and submandibular spaces and the presence of the inferior alveolar nerve. Two full-thickness flaps are reflected to access the underlying bone. The crestal incision needs to separate the residual keratinized gingiva in two equal vestibular and lingual portions. Posteriorly, the releasing incision must be made toward the anterior border of the mandibular ramus to avoid cutting the lingual nerve. Anteriorly, the vestibular incision must go around the mental foramen to preserve the inferior alveolar nerve and extend toward the symphysis for laxity without a releasing incision.
During implant surgery on the posterior region of the mandible, two main priorities must be taken into account when elevating flaps: pushing back the sublingual space rich in neurovascular structures and avoiding damage to the mylohyoid muscle, which would lead to communication between the oral cavity and the submandibular space. This could lead to a hemorrhage obstructing the upper aerodigestive tract.16 Placing axial implants is limited in the atrophic posterior mandibular region due to the proximity of the inferior alveolar nerve in the body of the mandible and the risk of nerve injury it could cause.
The Panthera SUB subperiosteal implant, shown below, is a viable treatment option in this situation. It is done in a single surgery: the proximity of the inferior alveolar nerve to the alveolar crest and the low bone volume available are not a contraindication.
Characteristics and design of the SUB implant
The Panthera SUB implant is produced by Panthera Dental (Québec) and was developed by Dr. Yvan Poitras (Québec).
Data collection is similar to that performed when planning axial implants:
- a CBCT
- a recording of the dental and mucosal surfaces
- a mock-up
The quality and precision of the CBCT are critical and the main factors determining how accurately the subperiosteal implant adapts to the bone surface. It is therefore necessary to optimize the dental X-ray equipment settings to obtain high-resolution images with enough contrast to visualize the bones in other structures. Moreover, a wide field allowing for a single pass of the molar zone to be implanted, the ipsilateral ramus posteriorly, and the symphyseal region up to the contralateral canine is a minimum requirement. Stitching (overlapping several “narrow-field” images) is strongly discouraged, given the risks of distortion. Finally, the data must be exported to the universal DICOM format.
A conventional physical impression that is later scanned by a laboratory scanner or a native digital image using an intraoral camera allows for initial dental and mucosal surfaces to be recorded. The file must be exported to STL or PLY format.
A physical or digital mock-up must match up with the dental and mucosal surfaces. The surgeon and technician use the protocol with which they are most familiar (fully digital workflow, dual scan with radiopaque markers, etc.).
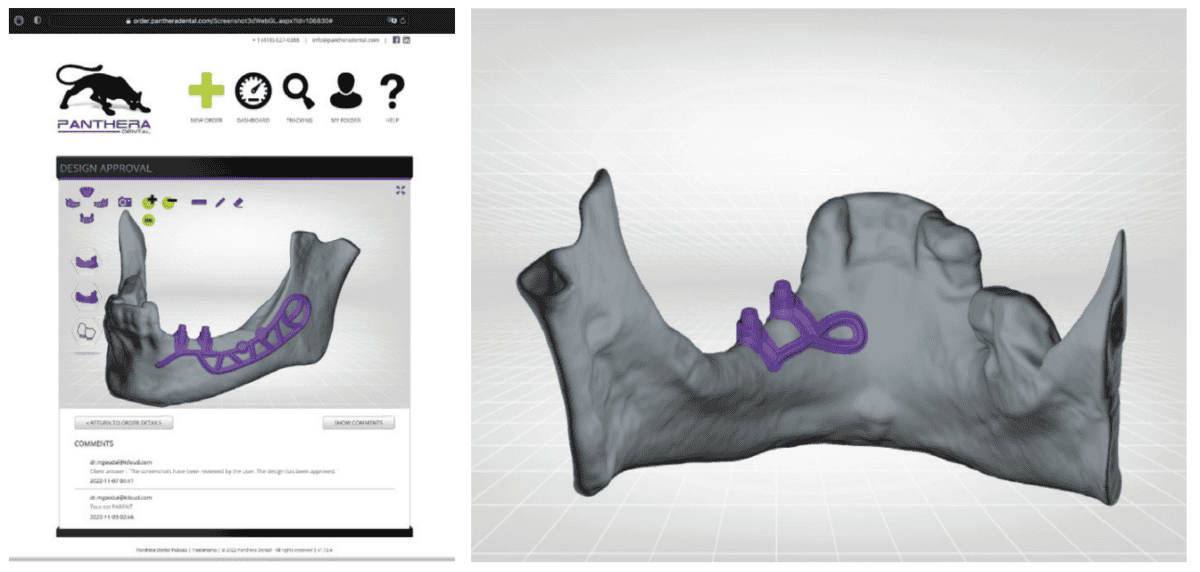
This data is recorded on the Panthera order platform. Using a simple step-by-step process, the clinician can indicate the number of teeth to be replaced, the desired position of the prosthetic platforms, etc. Once the order has been placed and the data sent, the dashboard can be used to track the progress of the work:
- confirmation of data receipt
- confirmation of data quality
- fusion of three-data layers
- implant design proposal
- validation by the surgeon
- implant production
- implant shipping
Panthera designers use proprietary software to perform a precise fusion of the three data types. The design is produced in-house according to the surgeon’s order and in accordance with the mock-up, all while following the same blueprint: In the vestibular region, the skeleton extends anteriorly by an arm going around the emergence of the inferior alveolar nerve, posteriorly by a loop up to the outer surface of the mandibular ramus. In the lingual region, the frame stops distally in vertical alignment with the most distal prosthetic platform and apically over the mylohyoid ridge. However, a loop extends the implant to the symphyseal region of the mandibular. Finally, the external oblique ridge, which is highly corticalized, is the anchoring location for osteosynthesis screws (Figures 2A and 2B).
After validation by the surgeon, five-axis CNC milling machines with a precision of 5 µm (far superior to the acquisition of the CT scan) produce subperiosteal implants in disks made of Ti6Al4V ELI (Grade 23), a titanium-aluminum-vanadium alloy that is purer than the standard Ti6Al4V alloy. After machining, the surface in contact with the bone and the periosteum is sanded.
The combination of the following three characteristics achieve greater results for subperiosteal implants compared to traditional techniques:
- biocompatible material
- precise adjustment (CT scan, CAD/CAM, machining)
- rough surface
Clinical case and planning
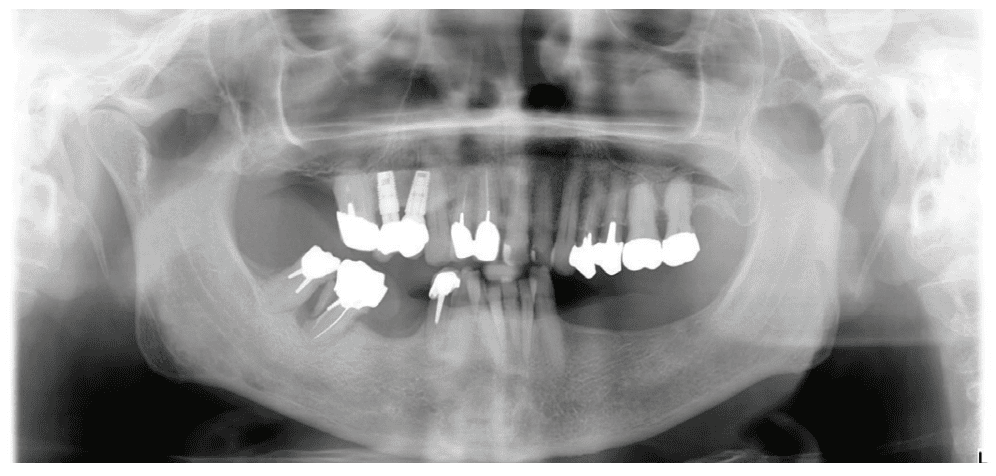
Our patient is consulting for pain in the right mandibular molar region and difficulty chewing (Figure 3).
Her history is quite common: discomfort, followed by a failure to wear the removable denture with a metal framework, and finally neglecting care for family reasons. At age 77, she is perfectly healthy enough for oral surgery. However, she would prefer not to undergo long and complex implant treatment. Her request is first and foremost functional. Esthetics and price are secondary concerns. We therefore offer the following treatment plan: keep the malpositioned anterior mandibular teeth with only mild gingivitis, rehabilitate the left posterior mandibular region with a subperiosteal implant, extract molars 47 and 48, and reassess the best implant solution for this region after healing.
Given the initial anatomical situation (strong resorption, significant mobile soft tissue, blockage by the tongue, V-shaped mandible), a conventional impression with a CIT and a physical mock-up with radiopaque markers are preferred.
Data is exported to the Panthera platform, and we receive a design proposal within a few days. The visualization tools allow us to scroll freely in the three-dimensional reconstruction area. Each element (implant, mock-up, bone) can be viewed separately, hidden, made opaque or clear (Figures 2A, 2B, 4A, 4B, and 4C). The proposal is validated by the surgeon for the implant to be produced and shipped.

Once it is received, the implant is cleaned, decontaminated, and sterilized at the dental office.
Surgical procedure
The procedure begins with local anesthesia at multiple points, vestibular and lingual, from the symphyseal region to the ascending ramus. However, an infiltration in the lingula of the mandible is not necessary. The incision is performed using the technique described above (Figures 5A and 5B).
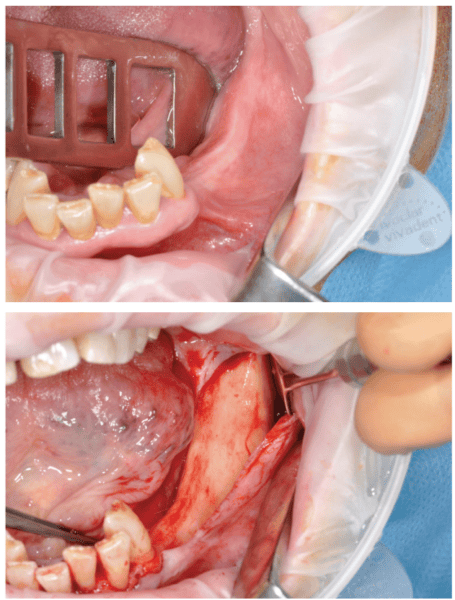
It is imperative to carefully reflect a full-thickness flap following the periosteum. After reflection, an atraumatic periosteal expansion using a soft brush (Figure 6) will allow for the flaps to be repositioned without tension over the implant and bony surfaces at the end of the procedure.

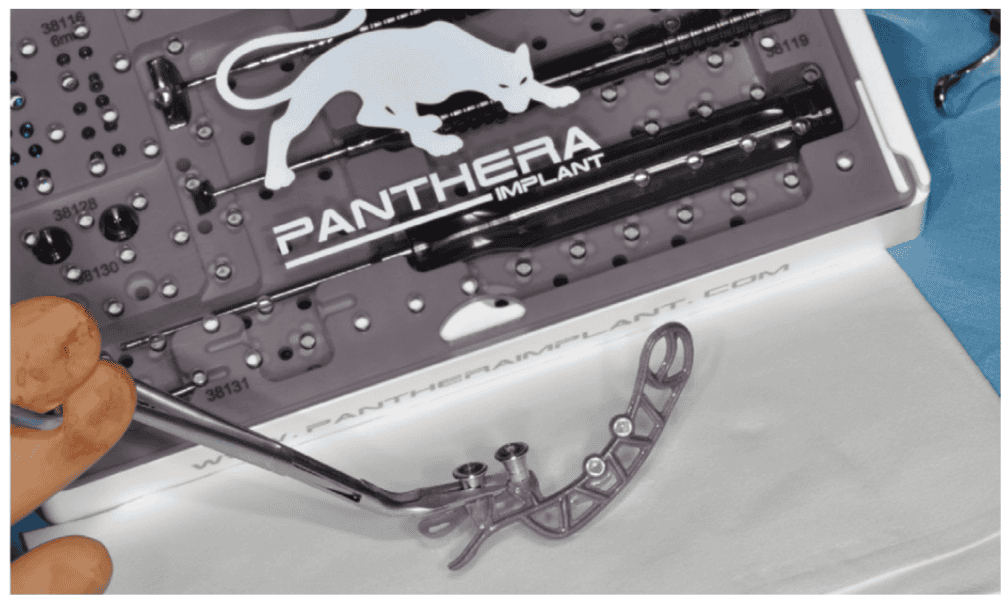
After the soft tissue is prepared, the bony surface is carefully cleaned. For easy insertion, the healing abutments are left in place, and the implant is held firmly with hemostatic forceps (Figure 7). The implant is inserted via distal translation in the direction of the angle of the mandible, then a mesio-anterior rotation. The surgeon must control the lack of mobility and the adaptation of the implant to the bony surface at all points (Figures 8A, 8B, 8C, and 8D).

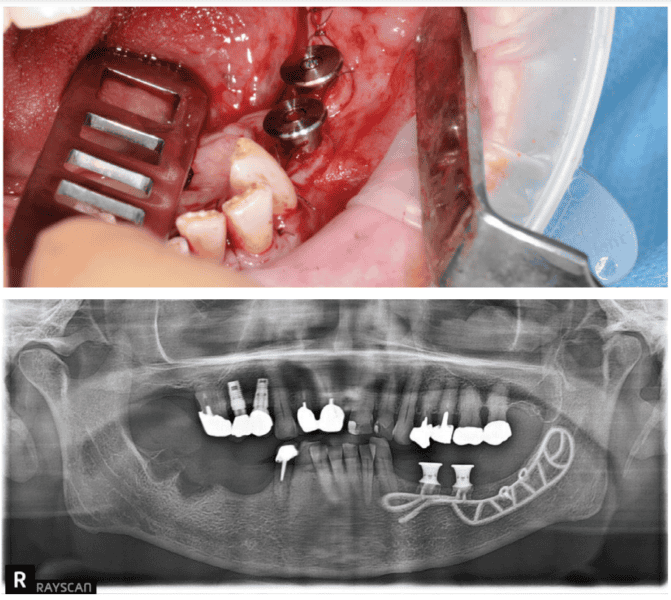
To ensure the implant is stable during the osseointegration period, an osteosynthesis screw is placed in the prepared space (Figures 9A, 9B, 9C, and 9D).
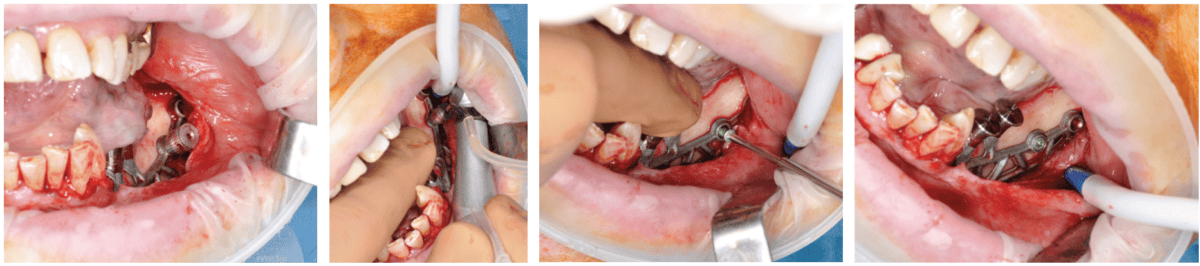
The flaps are carefully repositioned and sutured without tension with Halsted and over-and-over sutures (Figures 10A and 10B).
Healing and osseointegration
Osseointegration takes 4 months to complete and occurs through two mechanisms:
- First through direct contact of the bone with the rough titanium finish of the inner surface of the implant
- Next through progressive bone apposition on the equally rough outer surface. In fact, the passive repositioning of the flap at the end of the procedure creates a space between the periosteum (inner surface of the flap) and the implant placed over the bone where the blood clot will be trapped (Figure 11).17-19

The patient returns four months later for a clinical follow-up (Figures 12A and 12B) and X-rays (Figure 13).
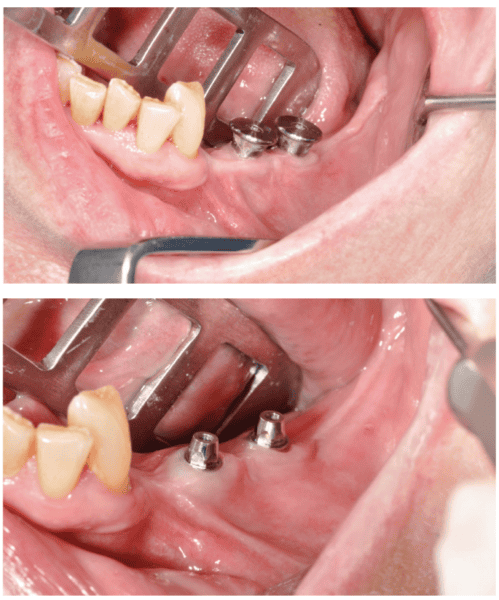

The permanent dentures are then placed over a titanium frame processed by Panthera Dental and stratified in composite at the denture laboratory (Figures 14A-14C).

Literature review and success rate
We are at the stage where we can see if the survival rates of subperiosteal implants have improved compared to more common techniques such as mandibular grafts for implant rehabilitation of atrophic posterior mandibular regions. The systematic literature review below compares the clinical results of these two techniques and justifies the use of CAD/CAM subperiosteal implants.
Materials and method
The literature review was performed using the PRISMA protocol criteria. Searches took place in March 2021 using the PubMed, DOSS, Embase, and Cochrane databases, and it was split into two parts:
- A search focused on mandibular subperiosteal implants using the following keywords: “subperiosteal implant” and (“CAD/CAM” or “3D printing” or “direct metallaser sintering” or “additive manufacture”) and “dental implantation, subperiosteal” [MeSH Terms] and “computer-aided design” [MeSH Terms].
- A search focused on inlay bone grafts using the following keywords: “mandible” and “vertical ridge augmentation” and “sandwich osteotomy” OR “inlay bone graft” or “interpositional bone graft” and “alveolar ridge augmentation” [MeSH Terms] AND “mandible” and “alveolar bone atrophy” [MeSH Terms] and “bone grafting” [MeSH Terms] OR “mandibular osteotomy” [MeSH Terms].
Results
These searches found 30 articles meeting the selection criteria for this literature review: five on subperiosteal implants20–24 and 25 on inlay grafts.25–49 By analyzing the results, we can measure the implant survival rate (number of patients who did not lose any implants/total number of patients). Among the 86 patients who participated in studies on subperiosteal implants, three lost an implant due to recurring infections. The implant survival rate between 8 months to 3 years is 96.5%. For inlay grafts, implant survival depends on the success of the graft. Among the 345 patients who participated in studies, 28 grafts failed, and therefore no implants could be placed. Two studies did not specify the number of patients, but rather the number of implants when calculating the survival rate. The number of patients therefore decreases from 345 to 250. Among these patients, 19 lost one or more implants, for an implant survival rate of 92.5% between 8 months and 5 years.
Discussion
Analyzing these articles shows promising survival rates for the rehabilitation of atrophic posterior mandibular regions using subperiosteal implants. These articles are few, and their level of evidence is low. Most are clinical case reports with few patients (less than 100) with short-term follow-ups. Long-term clinical studies with a high level of evidence are required to reaffirm the true success of subperiosteal implants in a clinical setting.
A number of elements were unable to be assessed in this review, including the implant success rate, which is a better predictor of the long-term efficiency of implant-supported rehabilitation. However, the few prosthetic and biologic complications reported in the study seem to indicate high success rates for subperiosteal implants. Compared to inlay graft techniques, these implants have the advantage of requiring a single surgery with a short healing period and few postoperative and prosthetic complications, making them a reliable and promising alternative.
Conclusion
Thanks to CAD/CAM, Panthera SUB subperiosteal implants solve most issues encountered (lack of adjustment, two procedures, etc.) with their traditional counterparts. Moreover, using biocompatible titanium instead of cobalt-chrome allows for a true osseointegration of the implant. Finally, the literature tends to show good results with this technique in treating posterior mandibular edentulation.
Read more about how the The CAD/CAM SUB Implant™ by Panthera Dental is adaptable to specific bone morphology here: https://implantpracticeus.com/panthera-dental-cad-cam-sub-implant-a-new-approach-part-1/
 Dr. Mathieu Goudal is a Doctor of Dental Surgery from the Faculty of Reims, France. He has an exclusive practice in Implantology, Surgery, and Periodontology AUI – Paris VII. Dr. Goudal has a University Diploma in Calcified Tissues, Biomaterials, and Implantology (INSERM) from the Faculty of Medicine of Angers (France), and a University Diploma in Surgery and Implant Prosthesis — Faculty of Odontology of Lyon (France). Dr. Goudal is also an International Team for Implantology (ITI) fellow, lead team member and study club director.
Dr. Mathieu Goudal is a Doctor of Dental Surgery from the Faculty of Reims, France. He has an exclusive practice in Implantology, Surgery, and Periodontology AUI – Paris VII. Dr. Goudal has a University Diploma in Calcified Tissues, Biomaterials, and Implantology (INSERM) from the Faculty of Medicine of Angers (France), and a University Diploma in Surgery and Implant Prosthesis — Faculty of Odontology of Lyon (France). Dr. Goudal is also an International Team for Implantology (ITI) fellow, lead team member and study club director.
 Dr. Cécile Bailly received her Doctor of Dental Surgery from Faculty of Odontology of Bordeaux (France).
Dr. Cécile Bailly received her Doctor of Dental Surgery from Faculty of Odontology of Bordeaux (France).
Disclosure: Drs. Mathieu Goudal and Cécile Bailly are not compensated in any way by Panthera Dental.
- Silvestri KD, Carlotti AE. Subperiosteal implant: serving the dental profession for over 50 years. R I Dent J. 1995 Spring;28(1):11-13, 23.
- Sconzo J. The complete mandibular subperiosteal implant: an overview of its evolution. J Oral Implantol. 1998;24(1):14-15.
- Schou S, Pallesen L, Hjørting-Hansen E, Pedersen CS, Fibaek B. A 41-year history of a mandibular subperiosteal implant. Clin Oral Implants Res. 2000 Apr;11(2):171-178.
- Bodine RL, Yanase RT, Bodine A. Forty years of experience with subperiosteal implant dentures in 41 edentulous patients. J Prosthet Dent. 1996 Jan;75(1):33-44.
- Nguyen TM, Caruhel JB, Khonsari RH. A subperiosteal maxillary implant causing severe osteolysis. J Stomatol Oral Maxillofac Surg. 2018 Dec;119(6):523-525.
- van Steenberghe D, Brånemark PI, Quirynen M, De Mars G, Naert I. The rehabilitation of oral defects by osseointegrated implants. J Clin Periodontol. 1991 Jul;18(6):488-493.
- Nefussi JR. Le volume osseux résiduel après extraction dentaire est-il prédictible? (Is the residual bone volume after tooth extraction predictable?) In: Mise en place chirurgicale et gestion des tissus muqueux péri-implantaires. (In: Surgical implementation and management of peri-implant mucosal tissues) p. 102‑
- Nefussi JR. Biologie et physiologie du volume osseux implantable. (Biology and physiology of implant bone volume.) In: EMC. Elsevier Masson SAS. Paris; 2011. p. 1‑ Medecine buccale (Oral Medicine); vol. 28.
- Hienz SA, Paliwal S, Ivanovski S. Mechanisms of Bone Resorption in Periodontitis. J Immunol Res. 2015;2015:615486.
- Cawood JI, Howell RA. A classification of the edentulous jaws. Int J Oral Maxillofac Surg. 1988 Aug;17(4):232-236.
- Pietrokovski J, Massler M. Alveolar ridge resorption following tooth extraction. J Prosthet Dent. 1967 Jan;17(1):21-27.
- Urban IA, Nagursky H, Lozada JL. Horizontal ridge augmentation with a resorbable membrane and particulated autogenous bone with or without anorganic bovine bone-derived mineral: a prospective case series in 22 patients. Int J Oral Maxillofac Implants. 2011 Mar-Apr;26(2):404-414.
- Guillaume B. Accroissement osseux préimplantaire par disjonction osseuse. (Pre-implantation bone growth by bone disjunction.) Inf Dent. 2004;86(1640).
- Khoury F, Hanser T. Three-Dimensional Vertical Alveolar Ridge Augmentation in the Posterior Maxilla: A 10-year Clinical Study. Int J Oral Maxillofac Implants. 2019 Mar/Apr;34(2):471-480.
- Laurentjoye M, Ella B, Caix P. La tête. (The Head) In: Anatomie tête et cou. (Head and Neck Anatomy) 2015e éd. Bordeaux: Bergeret; 2015. p. 3‑
- Coutant JC, Martin R, Huault L, Ella B. Chirurgie du lambeau lingual. (Lingual Flap Surgery.) Inf Dent. 24 avr 2019;(16/17):35‑
- Minichetti JC. Analysis of HA-coated subperiosteal implants. J Oral Implantol. 2003;29(3):111-116; discussion 117-119.
- Cohen DJ, Cheng A, Kahn A, Aviram M, Whitehead AJ, Hyzy SL, Clohessy RM, Boyan BD, Schwartz Z. Novel Osteogenic Ti-6Al-4V Device For Restoration Of Dental Function In Patients With Large Bone Deficiencies: Design, Development And Implementation. Sci Rep. 2016 Feb 8;6:20493.
- Claffey N, Bashara H, O’Reilly P, Polyzois I. Evaluation of New Bone Formation and Osseointegration Around Subperiosteal Titanium Implants with Histometry and Nanoindentation. Int J Oral Maxillofac Implants. 2015 Sep-Oct;30(5):1004-10.
- Cerea M, Dolcini GA. Custom-Made Direct Metal Laser Sintering Titanium Subperiosteal Implants: A Retrospective Clinical Study on 70 Patients. Biomed Res Int. 2018 May 28;2018:5420391.
- Mangano C, Bianchi A, Mangano FG, Dana J, Colombo M, Solop I, Admakin O. Custom-made 3D printed subperiosteal titanium implants for the prosthetic restoration of the atrophic posterior mandible of elderly patients: a case series. 3D Print Med. 2020 Jan 8;6(1):1.
- Cohen DJ, Cheng A, Kahn A, Aviram M, Whitehead AJ, Hyzy SL, Clohessy RM, Boyan BD, Schwartz Z. Novel Osteogenic Ti-6Al-4V Device For Restoration Of Dental Function In Patients With Large Bone Deficiencies: Design, Development And Implementation. Sci Rep. 2016 Feb 8;6:20493.
- Oren D, Dror AA, Bramnik T, Sela E, Granot I, Srouji S. The power of three-dimensional printing technology in functional restoration of rare maxillomandibular deformity due to genetic disorder: a case report. J Med Case Reports. April 2021;15(1):197.
- Gellrich NC, Zimmerer RM, Spalthoff S, Jehn P, Pott PC, Rana M, Rahlf B. A customised digitally engineered solution for fixed dental rehabilitation in severe bone deficiency: A new innovative line extension in implant dentistry. J Craniomaxillofac Surg. 2017 Oct;45(10):1632-1638.
- Bolle C, Felice P, Barausse C, Pistilli V, Trullenque-Eriksson A, Esposito M. 4 mm long vs longer implants in augmented bone in posterior atrophic jaws: 1-year post-loading results from a multicentre randomised controlled trial. Eur J Oral Implantol. 2018;11(1):31-47.
- Esposito M, Cannizarro G, Soardi E, Pellegrino G, Pistilli R, Felice P. A 3-year post-loading report of a randomised controlled trial on the rehabilitation of posterior atrophic mandibles: short implants or longer implants in vertically augmented bone? Eur J Oral Implantol. 2011 Winter;4(4):301-311.
- Felice P, Barausse C, Pistilli R, Ippolito DR, Esposito M. Five-year results from a randomised controlled trial comparing prostheses supported by 5-mm long implants or by longer implants in augmented bone in posterior atrophic edentulous jaws. Int J Oral Implant. 2019;12(1):25‑
- Felice P, Barausse C, Pistilli R, Ippolito DR, Esposito M. Five-year results from a randomised controlled trial comparing prostheses supported by 5-mm long implants or by longer implants in augmented bone in posterior atrophic edentulous jaws. Int J Oral Implantol (Berl). 2019;12(1):25-37.
- Esposito M, Barausse C, Pistilli R, Piattelli M, Simone SD, Ippolito DR, Felice P. Posterior atrophic jaws rehabilitated with prostheses supported by 5 × 5 mm implants with a nanostructured calcium-incorporated titanium surface or by longer implants in augmented bone. Five-year results from a randomised controlled trial. Int J Oral Implantol Berl. 2019;12(1):39‑
- Esposito M, Pellegrino G, Pistilli R, Felice P. Rehabilitation of postrior atrophic edentulous jaws: prostheses supported by 5 mm short implants or by longer implants in augmented bone? One-year results from a pilot randomised clinical trial. Eur J Oral Implantol. 2011 Spring;4(1):21-30.
- Felice P, Pellegrino G, Checchi L, Pistilli R, Esposito M. Vertical augmentation with interpositional blocks of anorganic bovine bone vs. 7-mm-long implants in posterior mandibles: 1-year results of a randomized clinical trial. Clin Oral Implants Res. 2010 Dec;21(12):1394-403.
- Felice P, Marchetti C, Iezzi G, Piattelli A, Worthington H, Pellegrino G, Esposito M. Vertical ridge augmentation of the atrophic posterior mandible with interpositional bloc grafts: bone from the iliac crest vs. bovine anorganic bone. Clinical and histological results up to one year after loading from a randomized-controlled clinical trial. Clin Oral Implants Res. 2009 Dec;20(12):1386-1393.
- Brandtner C, Borumandi F, Krenkel C, Gaggl A. A new technique for sandwich osteoplasty with interpositional bone grafts for fixation. Int J Oral Maxillofac Implants. 2014 Sep-Oct;29(5):1164-1169.
- Geng YM, Zhou M, Parvini P, Scarlat S, Naujokat H, Abraha SM, Terheyden H. Sandwich osteotomy in atrophic mandibles: A retrospective study with a 2- to 144-month follow-up. Clin Oral Implants Res. 2019 Oct;30(10):1027-1037.
- Marconcini S, Covani U, Giammarinaro E, Velasco-Ortega E, De Santis D, Alfonsi F, Barone A. Clinical Success of Dental Implants Placed in Posterior Mandible Augmented With Interpositional Block Graft: 3-Year Results From a Prospective Cohort Clinical Study. J Oral Maxillofac Surg. 2019 Feb;77(2):289-298.
- Felice P, Pistilli R, Lizio G, Pellegrino G, Nisii A, Marchetti C. Inlay versus onlay iliac bone grafting in atrophic posterior mandible: a prospective controlled clinical trial for the comparison of two techniques. Clin Implant Dent Relat Res. 2009 Oct;11 Suppl 1:e69-82.
- Laviv A, Jensen OT, Tarazi E, Casap N. Alveolar sandwich osteotomy in resorbed alveolar ridge for dental implants: a 4-year prospective study. J Oral Maxillofac Surg. 2014 Feb;72(2):292-303.
- Bianchi A, Felice P, Lizio G, Marchetti C. Alveolar distraction osteogenesis versus inlay bone grafting in posterior mandibular atrophy: a prospective study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008 Mar;105(3):282-292.
- Esposito M, Grusovin MG, Felice P, Karatzopoulos G, Worthington HV, Coulthard P. Interventions for replacing missing teeth: horizontal and vertical bone augmentation techniques for dental implant treatment. Cochrane Database Syst Rev. 2009 Oct 7;2009(4):CD003607.
- Starch-Jensen T, Nielsen HB. Sandwich osteotomy of the atrophic posterior mandible with interpositional autogenous bone block graft compared with bone substitute material: a systematic review and meta-analysis. Br J Oral Maxillofac Surg. 2020 Dec;58(10):e237-e247.
- Esposito M, Grusovin MG, Felice P, Karatzopoulos G, Worthington HV, Coulthard P. The efficacy of horizontal and vertical bone augmentation procedures for dental implants – a Cochrane systematic review. Eur J Oral Implantol. 2009 Autumn;2(3):167-184.
- Jensen OT. Alveolar segmental “sandwich” osteotomies for posterior edentulous mandibular sites for dental implants. J Oral Maxillofac Surg. 2006 Mar;64(3):471-475.
- Pelo S, Boniello R, Moro A, Gasparini G, Amoroso PF. Augmentation of the atrophic edentulous mandible by a bilateral two-step osteotomy with autogenous bone graft to place osseointegrated dental implants. Int J Oral Maxillofac Surg. 2010 Mar;39(3):227-234.
- Marchetti C, Trasarti S, Corinaldesi G, Felice P. Interpositional bone grafts in the posterior mandibular region: a report on six patients. Int J Periodontics Restorative Dent. 2007 Dec;27(6):547-55.
- Sohn DS, Shin HI, Ahn MR, Lee JS. Piezoelectric vertical bone augmentation using the sandwich technique in an atrophic mandible and histomorphometric analysis of mineral allografts: a case report series. Int J Periodontics Restorative Dent. 2010 Aug;30(4):383-91.
- Felice P, Iezzi G, Lizio G, Piattelli A, Marchetti C. Reconstruction of atrophied posterior mandible with inlay technique and mandibular ramus block graft for implant prosthetic rehabilitation. J Oral Maxillofac Surg. 2009 Feb;67(2):372-380.
- Felice P, Piana L, Checchi L, Corvino V, Nannmark U, Piattelli M. Vertical ridge augmentation of an atrophic posterior mandible with an inlay technique and cancellous equine bone block: a case report. Int J Periodontics Restorative Dent. 2013 Mar-Apr;33(2):159-166.
- Roccuzzo A, Marchese S, Worsaae N, Jensen SS. The sandwich osteotomy technique to treat vertical alveolar bone defects prior to implant placement: a systematic review. Clin Oral Investig. 2020 Mar;24(3):1073-1089.
- Elnayef B, Monje A, Gargallo-Albiol J, Galindo-Moreno P, Wang HL, Hernández-Alfaro F. Vertical Ridge Augmentation in the Atrophic Mandible: A Systematic Review and Meta-Analysis. Int J Oral Maxillofac Implants. 2017 Mar/Apr;32(2):291-312.
Stay Relevant With Implant Practice US
Join our email list for CE courses and webinars, articles and mores

