Dr. Dan Holtzclaw delves into the evolving history of transnasal implants and provides a look at new PLACATE guidelines to define appropriate candidates for the technique.
Dr. Dan Holtzclaw describes one of the newest methods of implant treatment
Background
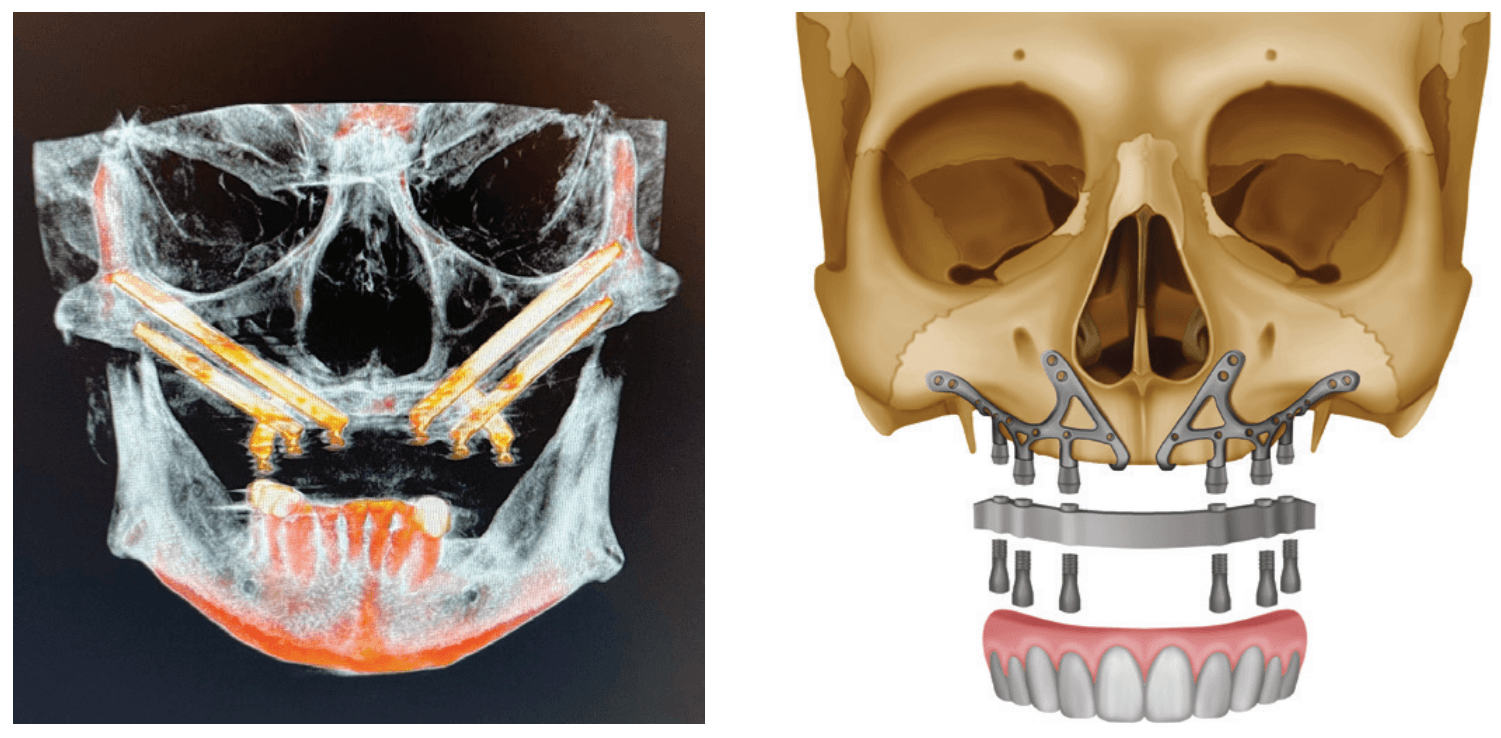
Treatment of severely atrophic maxillae often requires highly advanced procedures such as quad-zygomatic implants1-3 (Figure 1) or customized subperiosteal implants (Figure 2).4,5 Quad-zygomatic implant treatment has a long history of success, but requires significant surgical expertise due to limited malar bone availability and propinquity to anatomic structures such as the orbit and infraorbital nerve.6 Customized subperiosteal implants, on the other hand, are a promising new treatment option but have limited long-term follow-up data and significant expense.7 Transnasal dental implants have recently been introduced as another option for treatment of severely atrophic maxillae, specifically as an alternative to quad-zygomatic implant placement (Figure 3).8 Transnasal implants may serve as a replacement for anterosuperior zygomatic implants as they tangentially traverse the interior lateral nasal wall and achieve high insertion torque via 3 mm-5 mm of apical engagement in the confluence of the inferior concha, lateral nasal wall, and frontal process of the maxilla (Figure 4).8-16

In 2019, the first report on transnasal implants, called the Vanderlim technique, was published in Brazil as an alternative to the quad-zygomatic implant configuration.8 In this publication, the authors described using 16 mm–25 mm long implants placed tangentially along the interior of the lateral nasal wall to achieve insertion torque of 40-50 Ncm for immediate loading. In 2021, Almeida published a case report documenting use of an “extra-long transnasal implant” as an alternative to the quad-zygoma,10 and Vanderlim supported his 2019 publication with a series of 12 cases using “transnasal implants placed using the Vanderlim technique” with follow-up of 2-26 months.9 In 2023, Holtzclaw published a textbook with a case series of seven transnasal implant cases performed by himself and other dental implant surgeons.6
While there were no transnasal dental implant articles published in 2022, case reports on a handful of patients were published by Oh, et al.,12 and Sahin14 in 2023. In this same year, Holtzclaw published an article discussing protocols addressing atrophic maxillae which featured one case of unilateral transnasal implant treatment.17 In 2024, Sales echoed Holtzclaw’s 2023 publication with a case report on a unilateral transnasal implant in the treatment of an atrophic maxilla15 while Nunes, et al., published a case series of three patients treated with both unilateral and bilateral transnasal fixtures.13 Up to this point, all transnasal publications had been case reports or case series. This changed in late 2024 when Gelpi, et al., published a retrospective multi-center study of 45 transnasal implants placed in patients who underwent surgery between July 2021 and November 2023. In this largest study to date on transnasal implants, the survival rate was 100%, although mean follow-up was relatively short.
Initial guidelines for transnasal dental implant placement as noted in the initial publications by Vanderlim8,9 and Almeida10:
- Minimum bone volume of 3 mm for apical anchorage in the inferior concha and frontal process of the maxilla
- Minimum bone height of 4 mm between the ridge of the maxilla and the nasal cavity
- Insufficient premaxillary bone volume for the placement of two conventional implants
- Insufficient bone volume for the placement of two zygomatic implants in a single malar process
- Infraorbital nerve position which would be violated by placement of a zygomatic implant
- Large concavity of the anterior maxillary wall which may facilitate soft tissue recession with placement of a zygomatic implant
- Avoid placing transnasal implants in wide nasal cavities
- Avoid tearing the nasal mucosa during elevation
PLACATE guidelines
In 2023, Holtzclaw expanded the guidelines for transnasal dental implant placement with (P)re(LAC)rimal (A)ssesment of (T)ransnasal Implant (E)ngagement — PLACATE. 6 Under PLACATE guidelines, appropriate transnasal dental implant candidates must meet the following parameters:
- Simmen 2 or 3 classification of the nasolacrimal canal
- Prelacrimal bone width ≥3 mm
- Subnasal bone height ≥2 mm
- Vertical measurement from residual subnasal bone, or anticipated anterior alveolar ridge reduction level, to prelacrimal bone engagement point that does not exceed 25 mm
Failure to meet all four PLACATE criteria prevented a patient from being an appropriate transnasal implant candidate.

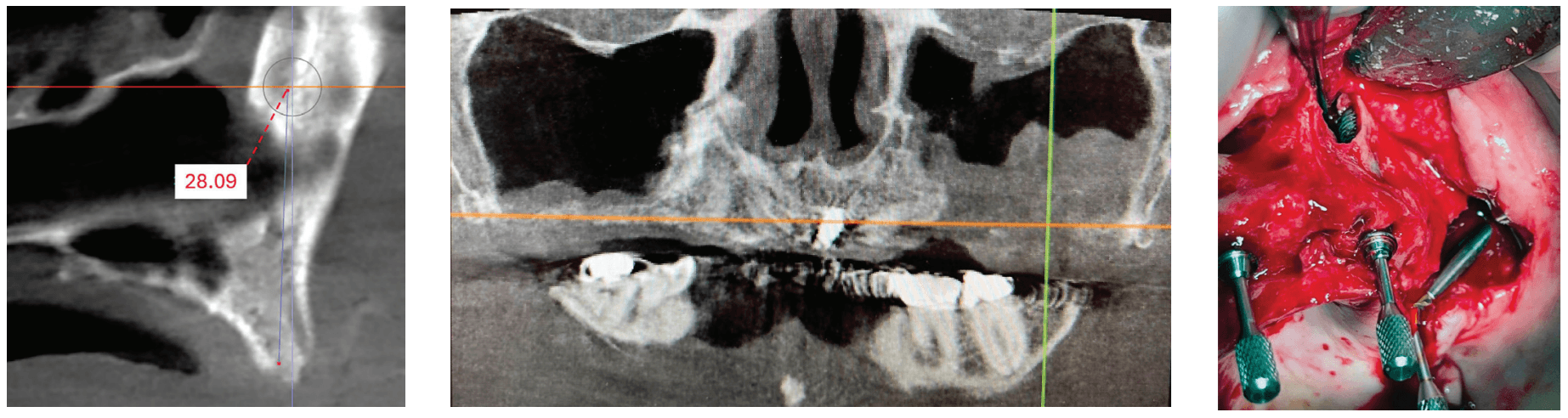
A recent 2025 retrospective review by Holtzclaw, et al.,11 evaluated anonymized cone beam computer tomography (CBCT) scans from 300 sequential referrals using PLACATE guidelines to determine transnasal dental implant feasibility. In this study, inferior conchae were initially located in the coronal plane, and imaging crosshairs were positioned just superior to this structure in the axial plane. To evaluate the ipsilateral and contralateral transnasal engagement points, imaging crosshairs were next positioned over each concha in the sagittal plane. This prelacrimal engagement point, sometimes referred to as the “Z-Point”,6,12 was then evaluated according to PLACATE guidelines as follows:
- Simmen classification19 determined by measurement from the external aspect of the frontal maxilla to the most anterior aspect of the nasolacrimal canal (Figure 5)
- Mediolateral measurement of prelacrimal bone width (Figure 6)
- Vertical measurement of subnasal bone height
- Vertical measurement from subnasal bone to prelacrimal bone engagement point (Figure 7)
The results of this study found that only 30.54% of patients qualified for transnasal dental implants anatomically. The most common disqualification was inadequate prelacrimal bone width which affected 49.71% of patients. Excessive subnasal bone height, which could foster placement of conventional dental implants, eliminated 28.74% of patients. The third most common reason for patient disqualification from transnasal dental implant placement, 22.16% of patients, was Simmen 1 classification which would result in potential violation of the nasolacrimal canal.
Case report
An 80-year-old male with a relatively clean medical history was referred for full-arch immediately loaded maxillary implant treatment. The patient had been previously treated with maxillary dental implants in a traditional All-on-X approach. The referring clinician noted that the patient’s bone was extremely “soft” and that insertion torque for most of the implants was very low. Although these implants were not immediately loaded, they ultimately failed and created large oroantral communications. While the communications were ultimately closed, extremely large defects resulted in the floor and walls of the maxillary sinuses (Figure 8). CBCT analysis revealed a significantly thickened left Schneiderian membrane and occluded osteomeatal complex. The patient was referred to ENT for a Functional Endoscopic Sinus Surgery (FESS) procedure. Upon healing, a new CBCT was taken and evaluated for potential treatment.
Due to the atrophic nature of the maxilla, treatment following the PATZi protocol was planned.6,17,20 CBCT evaluation revealed pterygomaxillary bone appropriate for pterygoid implants allowing for posterior arch support and cantilever elimination. The zygomas were of adequate height and width to accommodate multiple zygomatic implant fixtures bilaterally. PLACATE guidelines were used to evaluate the patient for potential treatment with transnasal implants. With Simmen 3 nasolacrimal canal classification, ≥ 3 mm of prelacrimal bone, ≥2 mm subnasal bone, and ≤ 25 mm to the Z-point, the patient satisfied all PLACATE parameters. Accordingly, a treatment plan of bilateral pterygoid, single zygomatic, and transnasal implants was agreed upon.
Following the induction of general anesthesia, extraoral and intraoral local anesthesia was applied. To avoid exposing the large subantral bony defects, mini-flaps were elevated at the pterygoid landing areas to expose the hamular notch. The pterygoid fossa was identified via probing, and pterygoid implant placement ensued. Following the PATZi protocol, bilateral pterygoid implants were placed first and both achieved insertion torque between 45+ Ncm.

Following PATZi, anterior support was sought next. As such, the nasal mucosa was elevated to expose the floor of the nasal cavity and the bone of the inferior conchae. A pair of 25 mm transnasal implants were placed, and each achieved high insertion torque of 45+ Ncm (Figures 9-11). Continuing with the PATZi protocol and treatment plan, 42.5 mm long zygomatic implants were placed in both zygomas. The zygomatic implants were placed using an extrasinus approach and both achieved insertion torque of 45+Ncm. Buccal fat pedicles were advanced bilaterally to cover extrasinus portions of the zygomatic implants, and flap closure was achieved with 4-0 chromic gut suture. The patient was immediately temporized with a screw-retained transitional bridge (Figure 12), and a final zirconia restoration was delivered after 8 months of healing (Figure 13).

Discussion
With fewer than 200 published cases and less than 7 years of follow-up, transnasal dental implants are one of the newest styles of treatment in implant dentistry. The limited number of studies which have evaluated this treatment have generally found transnasal implants to be of diameters ranging from 3.5 mm to 4.2 mm and lengths of 20 mm-25 mm.6,8-16 Having multicortical anchorage points in subnasal and prelacrimal bones, transnasal implants have been found to have high insertion torques appropriate for immediate loading.6,8-16 A unique feature of transnasal dental implants is that the midbody of the fixture remains exposed in the nasal cavity. Regarding exposed transnasal implant threads in the nasal cavity, there is currently no consensus on the need for grafting.
Although transnasal implants can be placed under direct visualization, their proximity to certain antatomic structures requires intimate anatomic knowledge and surgical skill. Iatrogenic damage to Kesselbach’s complex may result in excessive hemorrhaging while tearing of the nasal mucosa may lead to oronasal fistulae.6 Careless mucoperiosteal flap elevation can result in damage to the infraorbital nerve, and poor placement of transnasal implant fixtures may lead to dacryostenosis, epiphora, and dacryocystitis.6 Fortunately, to date, published studies have shown few complications with transnasal dental implants and few failures.
Conclusion
When anatomic conditions are appropriate, transnasal dental implants are a promising alternative to anterosuperior zygomatic implant fixtures in quad-zygo treatment. While continually emerging updates such as PLACATE guidelines are improving the safety and predictability of transnasal dental implants, more studies with longer follow-up times are needed to confirm the reliability of this relatively new treatment.
Transnasal implants can be an option with Dr. Holtzclaw’s PATZI protocol. Read more about treatment of severely atrophic maxillae using the PATZI remote anchorage protocol here: https://implantpracticeus.com/ce-articles/treatment-of-severely-atrophic-maxillae-using-the-patzi-remote-anchorage-protocol-a-case-series/. Subscribers can pass the quiz and receive 2 CE credits!
 Dan Holtzclaw, DDS, MS, is President of Holzklau Full Arch Implant Consulting and maintains practices limited to remote anchorage implantology in multiple states. He is a Diplomate of the American Board of Periodontology and Diplomate of the International Congress of Oral Implantologists. Dr. Holtzclaw has published over 60 articles in peer reviewed journals in addition to multiple textbooks. He served as the Editor-In-Chief of the Journal of Implant and Advanced Clinical Dentistry for 13 years in addition to serving as an editorial board member and/or editorial reviewer for several other dental journals.
Dan Holtzclaw, DDS, MS, is President of Holzklau Full Arch Implant Consulting and maintains practices limited to remote anchorage implantology in multiple states. He is a Diplomate of the American Board of Periodontology and Diplomate of the International Congress of Oral Implantologists. Dr. Holtzclaw has published over 60 articles in peer reviewed journals in addition to multiple textbooks. He served as the Editor-In-Chief of the Journal of Implant and Advanced Clinical Dentistry for 13 years in addition to serving as an editorial board member and/or editorial reviewer for several other dental journals.
Disclosure: The author reports no conflicts of interest with any products mentioned in this article. He is the developer of the HESIAn, PFAST, PLACATE, and PHARS protocols and co-developer of the PATZi protocol.
- Bothur S, Jonsson G, Sandahl L. Modified technique using multiple zygomatic implants in reconstruction of the atrophic maxilla: a technical note. Int J Oral Maxillofac Implants. 2003 Nov-Dec;18(6):902-904. PMID: 14696667.
- Varghese KG, Gandhi N, Kurian N, Daniel AY, Dhawan K, Joseph M, Varghese MG. Rehabilitation of the severely resorbed maxilla by using quad zygomatic implant-supported prostheses: a systematic review and meta-analysis. J Prosthet Dent. 2023 Oct;130(4):543-552. doi: 10.1016/j.prosdent.2021.11.007. Epub 2021 Dec 14.
- Lan K, Wang F, Huang W, Davó R, Wu Y. Quad Zygomatic Implants: A Systematic Review and Meta-analysis on Survival and Complications. Int J Oral Maxillofac Implants. 2021 Jan-Feb;36(1):21-29. doi: 10.11607/jomi.8417.
- Anitua E, Eguia A, Staudigl C, Alkhraisat MH. Clinical performance of additively manufactured subperiosteal implants: a systematic review. Int J Implant Dent. 2024 Feb 5;10(1):4. doi: 10.1186/s40729-024-00521-6.
- Onică N, Budală DG, Baciu ER, Onică CA, Gelețu GL, Murariu A, Balan M, Pertea M, Stelea C. Long-Term Clinical Outcomes of 3D-Printed Subperiosteal Titanium Implants: A 6-Year Follow-Up. J Pers Med. 2024 May 18;14(5):541. doi: 10.3390/jpm14050541.
- Holtzclaw D. Remote Anchorage Solutions for Severe Maxillary Atrophy: Zygomatic, Pterygoid, Transnasal, Nasal Rim, Piriform Rim, Nasopalatine, and Trans-Sinus Dental Implants. Austin, Texas: Zygoma Partners; 2023.
- Herce-López J, Pingarrón MDC, Tofé-Povedano Á, García-Arana L, Espino-Segura-Illa M, Sieira-Gil R, Rodado-Alonso C, Sánchez-Torres A, Figueiredo R. Customized Subperiosteal Implants for the Rehabilitation of Atrophic Jaws: A Consensus Report and Literature Review. Biomimetics (Basel). 2024 Jan 22;9(1):61. doi: 10.3390/biomimetics9010061.
- Vanderlim BC, Baptista D, Manfro R. Transnasal Implant (Vanderlim Technique) as an option to the second zygomatic implant. Solucoes Clinicas para Reabilitacoes Totais Sobre Implantes Sem Enxertos Osseos. 2019;12:199-215.
- Vanderlim BC, Baptista D, Almeida JR. Transnasal implants: Vanderlim technique as an alternative to the Zygoma Quad technique in atrophic total jaws – series of 12 cases in immediate load and follow-up of two to 26 months. Implant News. 2021;6(5):1-14.
- Almeida PHT, Cacciacane SH, Arcazas Junior A. Extra-long transnasal implants as alternative for Quad Zygoma: Case report. Ann Med Surg (Lond). 2021 Jul 27;68:102635. doi: 10.1016/j.amsu.2021.102635.
- Holtzclaw D, Zelig D, Bulot D, Nelson S, Nguyen A. Feasibility of Transnasal Dental Implant Placement Determined by PLACATE Guidelines. Dent Res Oral Health. 2025;8(1):21-26.
- Oh S, Zelig D, Aalam AA, Kurtzman GM. Case report: utilization of Z-Point fixture “Trans-nasal” implants. Ann Med Surg (Lond). 2023 Apr 11;85(5):1959-1965. doi: 10.1097/MS9.0000000000000520.
- Nunes M, de Araújo Nobre M, Camargo V. All-on-4 Hybrid with Extra-Long Transnasal Implants: Descriptions of the Technique and Short-Term Outcomes in Three Cases. J Clin Med. 2024 Jun 6;13(11):3348. doi: 10.3390/jcm13113348.
- Şahin O. Treatment of Severely Atrophic Maxilla by Using Zygomatic, Pterygoid, and Transnasal Implants. J Craniofac Surg. 2024 Mar-Apr 01;35(2):e145-e146. doi: 10.1097/SCS.0000000000009896. Epub 2023 Nov 20.
- Sales P, Amaral G. The use of the Transnasal implant associated with the zygomatic implants in the treatment of atrophic maxilla: A Case Report. Eur J Stomatol Oral Fac Surg. 2024;1(1):1-6.
- Montanari Dalmolin CA, Baptista D, Meurer E, Andretti F, Almeida Grossi JR, Vanderlim BC. A Transnasal Implant Technique. Inside Dent. 2023;19(6):22-26.
- Holtzclaw D. Treatment of Severely Atrophic Maxillae using the PATZI Remote Anchorage Protocol: A Case Series. Impl Prac US. 2023;16(4):26-32.
- Gelpi F, Alberti C, De Santis D, Bevilacqua M, Mellone F, Tealdo T. A Retrospective Multicentric Study of 52 Nasal and Transnasal Implants in 31 Severely Atrophic Patients to Reduce Anterior Cantilever Bending in Full-Arch Implant-Supported Fixed Rehabilitations. Int J Oral Maxillofac Implants. 2025 Feb 7;40(1):69-75. doi: 10.11607/jomi.10921.
- Simmen D, Veerasigamani N, Briner HR, Jones N, Schuknecht B. Anterior maxillary wall and lacrimal duct relationship – CT analysis for prelacrimal access to the maxillary sinus. Rhinology. 2017 Jun 1;55(2):170-174.
- Ponnusamy S, Gonzalez J, Holtzclaw D. A Systematic Approach to Restoring Full Arch Length with Maxillary Fixed Implant Reconstruction: The PATZi Protocol. Int J Oral Maxillofac Implants. 2023 Oct 17;38(5):996-1004. doi: 10.11607/jomi.10153.
Stay Relevant With Implant Practice US
Join our email list for CE courses and webinars, articles and mores

