Dr. Franck Renouard shares key insights from a presentation he gave at the Academy of Osseointegration (AO) 2014 Annual Meeting in a session called “Problem Solvers & Innovators”
 When reading this article, it’s important to remember that the scenario we are putting forward involves patients with low bone volume (vertical and/or horizontal) and that we are faced with choosing between two options: either to carry out a bone graft in order to place long- and/or wide-diameter implants or to place short/narrow implants without having to carry out a bone graft.
When reading this article, it’s important to remember that the scenario we are putting forward involves patients with low bone volume (vertical and/or horizontal) and that we are faced with choosing between two options: either to carry out a bone graft in order to place long- and/or wide-diameter implants or to place short/narrow implants without having to carry out a bone graft.
What is the difference between short/narrow implants and longer/wider ones with regards to competence and performance?
To reply to this question, we have to define the difference between competence and performance. Competence is the sum of knowledge and experience that a practitioner has acquired during the course of his/her career to date. Performance is the people’s capacity to use their competence in a given situation. For example, very competent surgeons’ performance will be negatively affected if they are stressed, tired, or are battling with personal issues that  are dominating their thoughts. The more complicated or complex the surgical procedure, the bigger the impact reduced performance will have upon the end result. To come back to our short/narrow implants, we can say that in order to place these implants, the practitioner must be competent, because these implants are often rather awkward to place due to low bone volumes. Still, for many practitioners, the use of these implants is a viable option. However, we have to say that bone grafting requires a greater degree of training and more extensive surgical experience. Likewise, if a practitioner’s performance is not up to his/her usual standard, this will have less of an impact on short/narrow implants than on longer or wider implants placed with the help of bone augmentation procedures. To sum up, error, which is an integral part of all human endeavor, will have less significant consequences if short/narrow implants are involved.
are dominating their thoughts. The more complicated or complex the surgical procedure, the bigger the impact reduced performance will have upon the end result. To come back to our short/narrow implants, we can say that in order to place these implants, the practitioner must be competent, because these implants are often rather awkward to place due to low bone volumes. Still, for many practitioners, the use of these implants is a viable option. However, we have to say that bone grafting requires a greater degree of training and more extensive surgical experience. Likewise, if a practitioner’s performance is not up to his/her usual standard, this will have less of an impact on short/narrow implants than on longer or wider implants placed with the help of bone augmentation procedures. To sum up, error, which is an integral part of all human endeavor, will have less significant consequences if short/narrow implants are involved.
What are the advantages of short/narrow implants?
Their main advantage is that they enable more practitioners to successfully take on cases they would previously not have had the skills to deal with. When there’s 7 mm of bone underneath a sinus, using short implants is an excellent alternative to the bone graft that would be required in order to place long implants. It’s the same with narrow implants and narrow alveolar ridges. Using these implants allows practitioners who have only limited surgical experience to work successfully with patients with narrow jawbones. An additional bonus with using narrow implants is that they make it easier to have adequate space between implants even when mesiodistal space is restricted. I often place two narrow implants when replacing premolars.
Are there limitations to the use of short/narrow implants?
The first limitation is obviously bone volume. I think that you need at least 6 mm for the maxilla and 8 mm for the mandible (above the inferior dental nerve for short implants). Narrow implants generally require at least 4 mm to 5 mm of alveolar ridge width. Another limitation for narrow implants is biomechanical in nature. Although all relevant literature is very encouraging with regard to this approach, given the extent of our knowledge about it at this moment in time, it is not a good idea to use this type of implant to replace single molars or canines in patients exhibiting canine-protected occlusion. Perhaps we should also be wary of adopting this approach when faced with patients who grind their teeth. There are also esthetic considerations. When bone resorption starts having an esthetic impact, a bone graft is needed. In this scenario, it would be better to use standard length implants.
What is the rationale behind the use of short/narrow versus longer implants? What are the key considerations guiding any such decision?
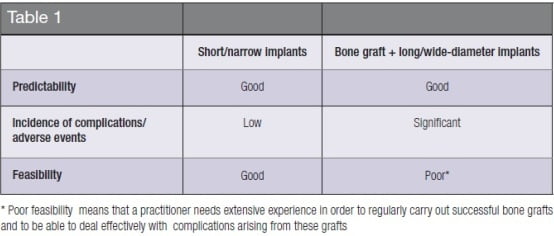
Once again, when we talk about the use of long-/wide-diameter implants, this means having to carry out a bone graft before or during the placing of implants. Choosing from these two options involves taking three criteria into account:
- To what extent is the outcome of the treatment predictable?
- What is the incidence of complications and adverse events of the treatment? (What are the consequences of the complications that I may encounter on implementing a given procedure?)
- How feasible is the procedure? (Am I capable of carrying out this procedure and managing any complications that may arise from it?)
We can summarize these three criteria in Table 1.
What human factors interfere with this decision-making process?
 Often practitioners are influenced by analytical biases and biases affecting how they make decisions. It is quite remarkable that in 2014, dentists persist in thinking that the longer the implant, the better its chances of long-term success, despite the widespread availability of scientific data to the contrary. This is known as confirmation bias. Once we have made our minds up about something, we find it very difficult to change them. We exhibit the same tendency when we only consider information that confirms our way of thinking and we reject information that challenges it, even when this data is substantial and reliable. This is a very human reaction, but it prevents us from making progress.
Often practitioners are influenced by analytical biases and biases affecting how they make decisions. It is quite remarkable that in 2014, dentists persist in thinking that the longer the implant, the better its chances of long-term success, despite the widespread availability of scientific data to the contrary. This is known as confirmation bias. Once we have made our minds up about something, we find it very difficult to change them. We exhibit the same tendency when we only consider information that confirms our way of thinking and we reject information that challenges it, even when this data is substantial and reliable. This is a very human reaction, but it prevents us from making progress.
Is the risk of complications higher with short/narrow implants?
If we take a broad perspective on the situation, we can say that placing short and/or narrow implants represents less of a risk than carrying out a bone graft and placing long and/or wide-diameter implants. Assessing the differences between the two approaches requires more than simply an examination of their respective success rates. It is also important to consider the consequences of failure, which are often more serious when bone grafts are involved. This relates to the incidence of complications and adverse events. This criterion was mentioned earlier. The major risk we run when using narrow implants is implant fracture, but seemingly this is a very rare occurrence.
What do you think the future holds for short/narrow implants?
I am convinced that more and more practitioners will start regularly using short or narrow implants. This is part and parcel of a wider movement toward simpler protocols. Our profession’s goal is to offer reliable, simple treatments to the widest possible range of people. Professor Per-Ingvar Brånemark once said that a good treatment had to be “Simple, available, affordable.” That says it all, really.
What type of patients are these implants particularly helpful for?
These implants are particularly helpful for patients exhibiting low levels of bone volume who are not suitable candidates for a bone graft, either for medical reasons, for financial reasons, or because they are afraid of what they see as major surgery.
References
1. Nisand D, Renouard F. Short implant in limited bone volume. Periodontol 2000. 2014; 66(1):72-96.
2. Renouard F, Charrier JG. Ewenn éd. The search for the weakest link. An introduction to the Human Factors. 2011.
3. Sohrabi K, Mushantat A, Esfandiari S, Feine J. How successful are small-diameter implants? A literature review. Clin Oral Implants Res. 2012;23(5):515-525.
Stay Relevant With Implant Practice US
Join our email list for CE courses and webinars, articles and mores

