
Dr. Paresh B. Patel illustrates a case that benefited from narrow diameter implants
For centuries, dentists have struggled to create a conventional complete denture that can satisfy the vast majority of patients in terms of retention, stability, and most importantly, function. It has been found that the average biting force for patients that have teeth is in the range of 150 to 250 psi.
That figure reduces by 50 psi soon after teeth are lost and reaches a staggering low of 5.6 psi after 15-plus years of struggling with dentures.
Up to 7 times more chewing strokes are required than a dentate patient. In addition to these deficiencies, the complete denture patient suffers from denture sores, reduced salivary flow, and iatrogenic resporbtion of the alveolar bone.
Most of these patients will not have the necessary width of bone to adequately accept the standard body implant with 1.5 mm of bone in all dimensions. Whether the patient is medically, financially, or anatomically compromised, the advent of the narrow body implant with a LOCATOR® attachment (Zest Anchors) allows the clinician to offer a widely accepted solution.
Narrow diameter implants (NDIs) typically can be placed in a flapless manner, greatly reducing surgical time, healing time, and patient discomfort. They also allow a greater number of patients who wish to have implant therapy to become candidates without additional surgical procedures that can potentially drive up economic costs.
Case history
 A 66-year-old male presented to our office with the chief complaint that his upper denture was no longer as retentive as it once was, even after a recent reline 2 months prior. He was opposing a lower implant-retained overdenture that was supported by four implants with the LOCATOR attachments. Although a visual exam showed an adequate maxillary ridge, upon performing a clinical exam, it was discovered that most of the tissue was mobile and unattached (Figure 1). Bone sounding demonstrated a highly thick area of tissue both buccal and lingual with a thin ridge of supporting bone. Due to these findings, a CBCT scan was ordered (i-CAT® FLX, Imaging Sciences International) (Figure 2). A dual-scan technique was prescribed as that would allow for two things: an accurate assessment of where the implants would emerge prosthetically, and that would also allow for the fabrication of a tissue-level surgical guide to minimize surgical trauma.
A 66-year-old male presented to our office with the chief complaint that his upper denture was no longer as retentive as it once was, even after a recent reline 2 months prior. He was opposing a lower implant-retained overdenture that was supported by four implants with the LOCATOR attachments. Although a visual exam showed an adequate maxillary ridge, upon performing a clinical exam, it was discovered that most of the tissue was mobile and unattached (Figure 1). Bone sounding demonstrated a highly thick area of tissue both buccal and lingual with a thin ridge of supporting bone. Due to these findings, a CBCT scan was ordered (i-CAT® FLX, Imaging Sciences International) (Figure 2). A dual-scan technique was prescribed as that would allow for two things: an accurate assessment of where the implants would emerge prosthetically, and that would also allow for the fabrication of a tissue-level surgical guide to minimize surgical trauma. 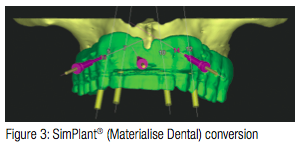 The CBCT scan file was then transmitted to 3DDX.com (3D Diagnostix) for conversion and treatment planning (Figure 3). Initially, four NDIs were planned from the clinical exam; however, with the added benefit of the i-CAT scan, two additional NDIs could be placed for a total of six implants to support a new maxillary overdenture. Six 2.9 x 12 mm Zest LOCATOR Overdenture Implants (LODI) were selected. This would allow for a low-profile attachment that self-aligns and would be compatible with what the patient was used to on his lower ridge. A tissue-level surgical guide was ordered and used to create the initial osteotomies with the 2.1 mm pilot bit (Figure 4).
The CBCT scan file was then transmitted to 3DDX.com (3D Diagnostix) for conversion and treatment planning (Figure 3). Initially, four NDIs were planned from the clinical exam; however, with the added benefit of the i-CAT scan, two additional NDIs could be placed for a total of six implants to support a new maxillary overdenture. Six 2.9 x 12 mm Zest LOCATOR Overdenture Implants (LODI) were selected. This would allow for a low-profile attachment that self-aligns and would be compatible with what the patient was used to on his lower ridge. A tissue-level surgical guide was ordered and used to create the initial osteotomies with the 2.1 mm pilot bit (Figure 4).  Due to the presence of soft bone, the self-tapping feature of the Zest LODI was utilized to compress and condense the bone. All six implants were inserted with the aid of an implant handpiece (Aseptico AEU-7000) (Figure 5). It is my preference to place the implants with a handpiece to avoid tipping or creating off-axis vector forces. Due to the excessive gingival tissue height, a 4-mm cuff height LOCATOR attachment was selected and was torqued to 30 Ncm (Figure 6). It is important to note that the implant packaging includes the LOCATOR and associated housing and inserts. A final CBCT scan was taken to ensure proper placement and confirm that the surgical guide was accurate (Figure 7).
Due to the presence of soft bone, the self-tapping feature of the Zest LODI was utilized to compress and condense the bone. All six implants were inserted with the aid of an implant handpiece (Aseptico AEU-7000) (Figure 5). It is my preference to place the implants with a handpiece to avoid tipping or creating off-axis vector forces. Due to the excessive gingival tissue height, a 4-mm cuff height LOCATOR attachment was selected and was torqued to 30 Ncm (Figure 6). It is important to note that the implant packaging includes the LOCATOR and associated housing and inserts. A final CBCT scan was taken to ensure proper placement and confirm that the surgical guide was accurate (Figure 7).
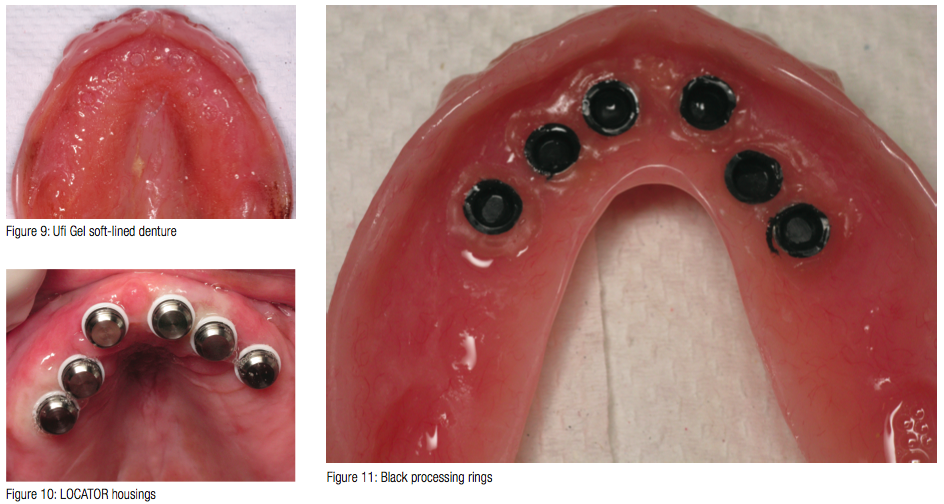
To create a totally passive fit of the existing denture areas that would require relief was identified with the use of Fit Test (VOCO America) (Figure 8). The process was repeated until no show-through areas of pink were observed. The denture was then cleaned and soft-lined with Ufi Gel (VOCO America). This would allow for an intimate fit of the denture against the tissue while the implants osseointegrated and the new overdenture was being fabricated (Figure 9).
At the final delivery appointment, the newly constructed overdenture was tried-in and verified for passive fit. All six housings were placed over the LOCATOR attachments (Figure 10) and were picked up chairside with the use of a self-cure material Quick Up (VOCO America) (Figure 11).

Utilizing NDI-supported overdentures can provide a better quality of life for most patients. The use of CBCT and surgical guides significantly reduce surgical and healing time as well as postoperative healing. Those patients that otherwise would not be ideal candidates for a standard body implant can now be offered an alternative to the O-ball style mini dental implant.

Stay Relevant With Implant Practice US
Join our email list for CE courses and webinars, articles and mores
