Dr. Dean C. Vafiadis reviews the significant contribution of digital dentistry to implant procedures for better diagnostic techniques and implementation
Educational aims and objectives
This article aims to discuss the various options and benefits regarding digital technologies
available to dentists who provide implant procedures.Expected outcomes
Implant Practice US subscribers can answer the CE questions to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
- Realize the various benefits of intraoral impressions with and without in-office milling.
- Identify various software programs available to facilitate implant placement.
- Recognize the possible uses for CBCT imaging in the implant process.
- Recognize how merging information in digital STL files and DICOM files can facilitate sharing data with the dental laboratory.
Over the past 10 years, digital dentistry has made a significant contribution to our profession. It has allowed the clinician better diagnostic techniques and allowed us to view the head and neck area from a different vantage point.1,2 We have broadened our diagnostic capabilities from using cone beam CT scans of the bony architecture to milling restorations for placement in a one-visit protocol. But which systems are best for your practice? The real answers lie in the training of these high-tech software and milling machines. The good news is that all the manufacturers and laboratories have made an educational and financial commitment to help clinicians make the right decision.
Intraoral impressions with in-office milling

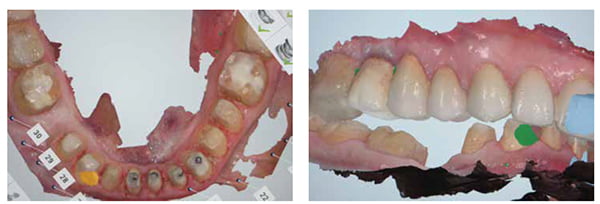
The first question to ask for your specific clinical private practice is, What kind of digital platform do I want to have? Does your office have the space to house a milling machine, and do one-visit restorations fall into your specific patient demographic? If so, then your choices are the CEREC Omnicam system (Sirona Dental Systems, New York) the NEVO-E4D (Planmeca E4D, Richardson, Texas), and the Carestream CS 3500 system (Carestream Dental LLC, Atlanta, Georgia). These scanning and milling technologies have made multiple upgrades that make scanning and milling possible within minutes and a total patient-specific restoration, even an anterior central veneer or crown, from scanning to insertion in under 90 minutes.3 The ceramic material by Ivoclar Vivadent® and 3M that is available has also been upgraded and provides very lifelike natural esthetics, good enough for even anterior central incisors (Figures 1-3). This comes with a large financial investment from the clinician, but the financial plans that are available can make this decision a comfortable and affordable 6-year payout. The laboratory costs, materials, and supplies used with conventional impressions will be huge savings for the practice. In most offices and clinics, the savings will offset some of the cost of the payment. For example, a $120,000 investment over 6 years may average around $2,000 per month. But the lab costs saved may be around $1,000 per month, and the supplies and materials savings may be $300. In addition, the savings of time and the second appointment will pay for the initial financial investment over the course of the year. The one-visit in-office CAD/CAM financial model will definitely save the clinician the cost of labs, materials, provisionals, trays, and countless hours of saved appointments. When looking at the office’s financial profit and loss columns, the practice saves thousands of dollars over the course of the 5-year payout. In addition, this provides the patient with a one-visit dental experience.4 The good news is after the unit is paid off, the financial gains really manifest to the bottom line of the practice. Although the technology is constantly changing, the scanners are still useful and will probably need upgrades every 2-3 years. Asking for this and cost differentials of “trade-in” packages ahead of time is a good idea. Also, the quality of the dentistry improves due to better preparation, margination, and the reduction of remaking impressions or remaking crowns because of quality control of the clinician and more accurate occlusal reduction.

Intraoral impressions without in-office milling
Due to the cost of scanning and in-office milling, some clinicians have decided that simply scanning will save them the cost of making a restoration and avoiding the goopy mess of regular PVS impression materials, which is what patients always complain about. Enter the intraoral scanners: 3Shape TRIOS® (3Shape Dental, Warren, New Jersey); 3M™ True Definition scanner (3M ESPE Dental, St. Paul, Minnesota); iTero® scanner (Align Technologies, San Jose, California). All these allow accurate impressions for any restoration, posterior, anterior, and full arch. Although there are other scanners available and more being manufactured in Europe and Asian markets, these have not yet made it into the U.S. market (Figures 4-5). A recent article was published that made a very detailed comparison with 10 different intraoral scanners but could not give a definitive answer as to which, if any, were better than another.4


The orthodontic community has readily adapted the iTero due its collaboration with Invisalign®. They can very abruptly take impressions and merge the files with the orthodontic software to create models and treatment plan for the orthodontic patient. But the others are soon to follow that digital orthodontic model. The accuracy of these new scanners is unprecedented, and the integration with the laboratory component has never been easier. The 3Shape Trios scanner is one of the fastest scanners available. It is easily integrated into any dental office. In single-provider dentists, group practices, or dental clinics, it can quickly be used for any restoration. In addition, the staff can be trained to take the intraoral impressions for diagnostic models, final impressions, and full arch impressions. Can you imagine that you could take a full arch impression to restore a full arch of restorations, a digital occlusal record in MIP position, and a counter scan in under 4 minutes? This is the average setting time of most PVS impressions. Then within 7 working days, you can have copings or even final restorations made at the highest level of accuracy and ready for delivery. One of the main advances in digital dental technology has been made possible by using printed models or stereolithography (SLA), instead of stone casts. Figures 6A-6D are examples of a printed model.

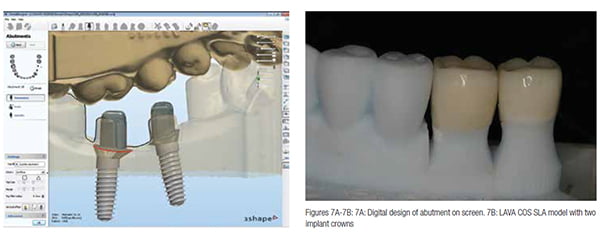
The printed models have been shown to accuracy levels of 30-50 microns, can be printed in less than 10 minutes, and with zero expansion, unlike dies and stone casts. This allows the technicians to really adapt the margins, interproximal contacts, and occlusal relationships on the computer monitor and deliver close to perfect restorations in any type of material, whether it be ceramo-metal, lithium disilicate, zirconia/feldspathic, or even gold crowns for the purist. An example of the screen shots used by the 3Shape designer software is shown in Figures 7A-7B.
Implants and digital technology
Want to place your own implants? Software programs such as Materialise (Materialise Plymouth, Michigan), Anatomage (Anatomage, San Jose, California) and SIMPLANT® (Dentsply, Waltham, Massachusetts), as well as many others, can diagnose the best possible placement angle, depth, width size, and type of implant that you desire. With the help of a CBCT scan and a trained laboratory technician, you can virtually look at the surgical plan and “print” a perfect surgical guide that actually fits within 4 business days. Placement of implants through flapless techniques better preserve the gingival tissues and allow the clinician ideal accuracy within a 100 micron tolerance for surgical placement. The digital workflow from surgical guides to final restoration can now be entirely done on the computer screen and verified instantly by a portable mobile device or tablet by the lab or clinician (Figures 8-11).


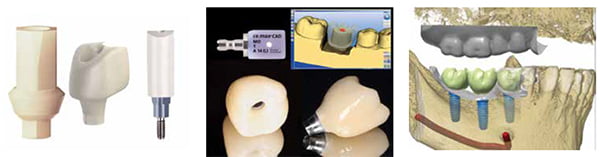
After the implants are healed, it’s really simple to fabricate your ideal CAD/CAM patient-specific abutments with digital scanned healing abutments such as Encode® (BIOMET™ 3i, Palm Beach Gardens, Florida). These have been around since 2004 and have cornered the market on digitally design CAD/CAM abutment fabrication.5,6 They are site-specific and patient-specific. They create ideal contoured and anatomically shaped abutments to replace the root and gingival form of the tooth that has been lost without removing them to take a fixture-level impression (Figures 12-15). For those not using the Encode system from BIOMET, there is a vast choice of scan bodies for all the other implant systems. These are made for each specific implant and size for the specific manufacturer, such as BioHorizons®, Straumann®, Ritter™, and MegaGen implants. They have their own scan bodies for their implant line. However, because of the high demand from the laboratories, independent companies have fabricated their own scan bodies that are available for each implant system, such as Elos Medtech (elos.com) and Bio-Dent (biodent.com) (Figure 16). These can be scanned for any implant being used and create a custom CAD/CAM abutment for ideal design. Some scanners are allowing clinicians to mill their own abutments, but this requires specific technical abilities that many clinicians are not comfortable with. I believe this will be a market that will soon get increase popularity, again only to minimize cost and time (Figure 17).
Merging of digital files
Another emerging technology is at the forefront with digital information. That is the merging of digital STL files and DICOM files. DICOM is a common file format, allowing utilization of the information between different platforms and manufacturers’ units. This allows the practitioner to have a specific scanner, for example, and the lab to have different software and still permit communication between the dentist and lab. This allows the laboratories to use open platform information and merge different software within one program (Figure 18). If it sounds like a “space-age concept,” well, it is. This has been available only within the past 3 years in the dental market but has been used by the U.S. NASA space program for over 15 years. The manufacturers have realized the potential to capture all esthetic dentists as well as implant dentists, and to do that, they had to open their software platforms to allow labs to use them with any digital software design system. This allows the lab techs to merge files from various scanners and milling systems to idealize every patient treatment, from implant placement to digital guides, and provisional materials such as polymethyl methacrylate acrylic (PMMA). In addition, with the new digital design systems that are available, the clinician can take a digital impression and fabricate ideal smile design with a printed digital wax-up that is available with the 3Shape software. For example, think about a 10-unit bridge on teeth or implants. The clinician would like to evaluate the placement of abutments, so that interproximal space is available. Utilizing two individual software programs (3Shape and Materialise), the laboratory can merge the scan of the provisional, which is superimposed onto the implant abutments or prepared teeth. Utilizing the provisional, the technician and clinician can review the proposed position of the final porcelain and restorations on a personal device or smartphone and in minutes communicate whether to continue or fine-tune the proposal. So with one image, the clinician can see the preparations or abutments, evaluate the frame to be milled, and see the final restorative position, all at the same time, and looking at exact occlusal contacts to be designed (Figures 19-20). This has been a dream of many of us for years — finally, a program that lets us see everything in one view, accurately and clearly to all members of the restorative and surgical team.

Diagnostically, this is an amazing breakthrough, especially for quality control. Using these programs, the labs can now design and fabricate restorations, surgical guides, partial and complete dentures, working smile designs, frames, and arches without depending on one certain scanner or software system. The dentists are free to make the best decision for their practices and not worry about their favorite labs purchasing software from the same company. This allows the laboratories to deliver excellent restorations regardless of the scanning system and platform that are provided. This gives a long awaited freedom to the clinician and maximizes efficiency for the labs. Of course, time for the patient and clinician is reduced as well as the cost of fabrication.
Many people ask, Why this massive change in the dental world? This all began when the cost of gold and precious metals reached record highs, and the cost of making a dental restoration was becoming prohibitive. Add labor costs to this, which account for a large percent of lab costs, To keep costs down, CAD/CAM technology allows high precision while allowing the lab to keep fees down and still generate a profit for the lab. This began a wave of corporate decisions from every dental company to create a digital platform within their business model. A rampant change in the profession also followed that utilized high-strength ceramics and materials that have allowed the low- as well as high-income practices to deliver excellent restorations for their patients. Like all things, change equals growth in different areas, and we have seen the collaboration of corporations, laboratories, and clinicians, where patients will finally benefit from this amazing and ever-changing technology. We must also give credit to the wonderful touchscreen phones and computers that have influenced all of our lives. It’s not difficult to realize that they would eventually infiltrate the medical and dental profession.
What is the future?
How much better can it be? Let’s think about what we do every day, and how we can make it better. Take, for instance, and extraction of a single tooth. This treatment is performed every day all around the world. What if we could scan the tooth and the root before extraction and have a duplicate root form of the exact shape and size ready at the time of surgery? In addition, what if it was made out of titanium and a high-grade surface texture with lateral side screws that could engage bone? How would the tissue response be to that surgical site? How would the loads be transferred with the exact anatomy of the root for that patient? Basically, every scenario of every procedure we do can be performed digitally. The ideas are only paralleled with one’s imagination, and my prediction is that our young dental professionals will push the envelope even more to where “no one has gone before.”
Digital technology reference sites
3M™ True Definition Scanner: solutions.3m.com
3Shape Trios® Scanner: www.3shapedental.com
Align Technologies / iTero Scanner: www.itero.com
BIOMET 3i™, Zimmer/Biomet Co. Bellatek Encode System: www.biomet3i.com
Carestream CS 3500 scanner: www.carestreamdental.com
Planmeca / E4D Technologies / NEVO scanner: www.e4d.com
Sirona / CEREC Omnicam: www.sirona.com
Materialise 3D Software: www.materialise.com
As always in technology, we are faced with the decision to be the first, follow a friend, or wait and see which is the best choice. It seems clear that regardless of the platform one chooses, it will no doubt impact the practice, the employees, and the overall patient experience. Digital dentistry is here, and it’s exciting. Sometimes you have to jump right in and swim!
Stay Relevant With Implant Practice US
Join our email list for CE courses and webinars, articles and mores

