Drs. Bradley S. McAllister, V. Thomas Eshraghi, and Hector F. Rios discuss the implant application of CBCT technology as reported in the consensus
Educational aims and objectives
This article aims to explain “Best Evidence Consensus on Cone Beam Computed Tomography: The Use of CBCT in the Management of the Patient Requiring Dental Implants,” which focuses on the consensus findings on the implant application of CBCT technology.
Expected outcomes
Implant Practice US subscribers can answer the CE questions to earn 2 hours of CE from reading this article. Take the quiz by clicking here. Correctly answering the questions will demonstrate the reader can:
- Identify how CBCT is used in the management of the patient requiring dental implants.
- Understand how CBCT technology can be used for guided implant surgery.
- Realize the benefits of CBCT for anatomical characterization.
- Realize how CBCT affects diagnosis and treatment outcome assessments.
Abstract
The October 2017 issue of the Journal of Periodontology includes the findings of an American Academy of Periodontology (AAP) best evidence consensus (BEC) meeting on cone beam computed tomography (CBCT) that was held in early 2017.1-4 The consensus meeting sought to answer three important clinical questions on the use of CBCT technology:
1. How is CBCT used in the management of the patient requiring dental implants?
2. When is CBCT imaging appropriate for diagnostic inquiry in the management of inflammatory periodontitis?
3. How is CBCT used in risk assessment of the dentofacial bone changes influenced by tooth movement (interdisciplinary periodontics/orthodontics)?
The purpose of this article is to give a brief overview of “Best Evidence Consensus on Cone Beam Computed Tomography: The Use of CBCT in the Management of the Patient Requiring Dental Implants,”1 which focuses on the consensus findings on the implant application of CBCT technology.
Introduction
With the BEC meetings, the AAP sought to develop a new conference model for emerging fields, such as CBCT, which enjoy widespread use but may not have sufficient research to create a traditional evidence-based review. Specific clinically relevant questions were developed, reviews were written, and then a panel of experts reviewed the findings and added expert opinion to help guide the clinician on use of CBCT technology. While implant reconstructions are clearly one of the largest applications for CBCT technology, many other specialists have found the modality to be a critical part of their armamentarium. In fact, other professional societies have addressed specific scenarios regarding when their members should consider using CBCT. In 2015, the original 2010 joint position statement from the American Association of Endodontists (AAE) and the American Academy of Oral and Maxillofacial Radiology (AAOMR) was updated to include recommendations for when limited field of view CBCT “should be considered the imaging modality of choice” during diagnosis, initial treatment, retreatment (nonsurgical and surgical), and special conditions.5 In 2016, their statement was revised once again with an additional recommendation regarding CBCT, stating: “In the absence of signs and symptoms, if limited FOV CBCT was the imaging modality of choice at the time of evaluation and treatment, it may be the modality of choice for follow-up evaluation.”5
With the many different applications for CBCT technology within periodontology6 and the rapid expansion of CBCT use across all dental specialties, it is clear why the AAP’s best evidence consensus is so important. Implementation, use and support of CBCT in the field have led to many studies on its effectiveness. The AAP best evidence consensus on implants nicely takes into consideration this new research in order to give an overview of the different ways CBCT currently applies to implant dentistry. Rios and colleagues found 559 reports when searching CBCT/Implant PubMed publications for the past 16 years.1 Of these, 161 were determined to be relevant to the purpose of their CBCT implant review. From that existing research, three distinct areas were identified where CBCT could be used in regard to implant dentistry:
• CBCT for diagnosis and treatment outcome assessments
• CBCT for use during treatment planning
• CBCT for anatomical characterization
 Figure 1: This CBCT rendering taken with a CS 9300 demonstrates the significant bone destruction on teeth Nos. 29 and 30, helping the clinician determine the treatment plan and best flap design for treatment
Figure 1: This CBCT rendering taken with a CS 9300 demonstrates the significant bone destruction on teeth Nos. 29 and 30, helping the clinician determine the treatment plan and best flap design for treatment
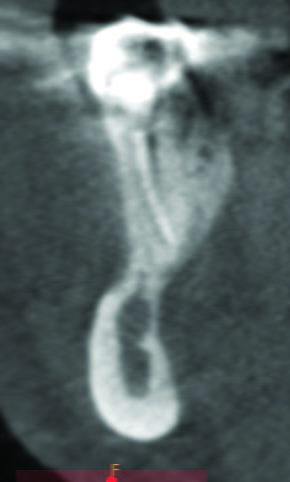 Figure 3: In this preoperative CBCT image, taken of fractured tooth No. 28, the image shows the absence of a buccal plate, the significant lingual undercut, and it identifies the inferior alveolar nerve allowing for accurate treatment planning of a challenging immediate implant case.
Figure 3: In this preoperative CBCT image, taken of fractured tooth No. 28, the image shows the absence of a buccal plate, the significant lingual undercut, and it identifies the inferior alveolar nerve allowing for accurate treatment planning of a challenging immediate implant case. Figure 2: The CBCT cross-sectional slice from the case in Figure 1 shows the buccal bone loss, intact lingual plate, and exactly where the inferior alveolar nerve resides in relation to the tooth
Figure 2: The CBCT cross-sectional slice from the case in Figure 1 shows the buccal bone loss, intact lingual plate, and exactly where the inferior alveolar nerve resides in relation to the tooth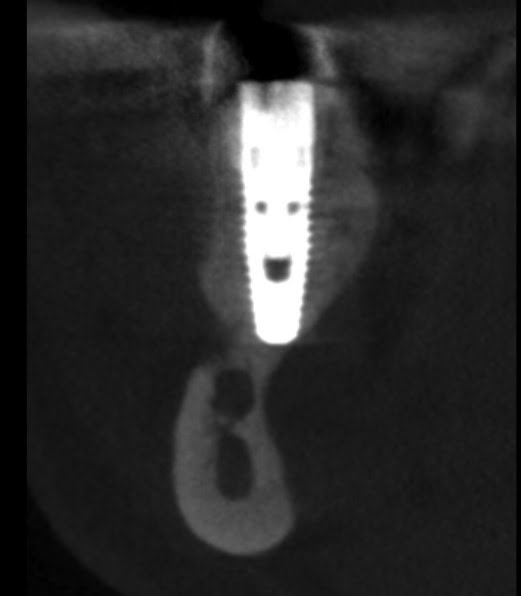 Figure 4: In this postoperative CBCT image of the completed immediate implant case shown in Figure 3, the buccal bone graft can be identified, and the appropriate implant proximity to the inferior alveolar nerve can be accurately verified
Figure 4: In this postoperative CBCT image of the completed immediate implant case shown in Figure 3, the buccal bone graft can be identified, and the appropriate implant proximity to the inferior alveolar nerve can be accurately verified
CBCT for diagnosis and treatment outcome assessments
The studies reviewed for this section examined the effectiveness of CBCT for diagnosis before and after implant therapy. In these studies, CBCT was used to evaluate the site of the future implant before placement to identify unusual pathologies and to confirm bone quality, quantity, and proximity to vital anatomy (Figures 1-4). “Treatment outcome assessments” refers to the use of CBCT after treatment to evaluate the success and overall quality of the implant placement.
Pathology/incidental findings
Due to the high frequency of incidental findings outside of the initial purpose of the CBCT scan, studies in this category stressed the importance of scans being thoroughly reviewed within and beyond the area of interest. Common incidental findings include osseous or sinus pathology, intracranial or vascular calcifications, and airway asymmetry, to name just a few. One study found airway narrowing and asymmetry to be the most common incidental finding at 35%, with dental developmental anomalies and other pathology being the least common (0.7% and 0.1%, respectively).7 Of these incidental findings, 16.1% required intervention, and 15.6% required monitoring.7 The studies confirmed that based on the high volume of incidental findings — greater than 90%, many agreed — CBCT scans should be carefully reviewed by someone proficient in the field of CBCT analysis.7-12
Peri-implantitis/implant fate
A current topic of research is whether CBCT could be used more effectively than 2D radiographic imaging methods to evaluate implant health and whether that evaluation could affect treatment outcomes. Monitoring the bone and tissue condition around dental implants is essential not only during follow-up evaluation under functional loading, but also during the assessment of strategies for regenerating lost peri-implant bone. Using specific strict imaging protocols, periapical radiographs can assess mesial and distal peri-implant bone levels under the right conditions.12 Other studies found benefits to using CBCT, such as reducing scattering artifacts, when compared to medical CT.14 While CBCT is a useful diagnostic tool for evaluating advanced peri-implantitis defects in some cases, most studies confirmed that PAs remain an effective method for measuring bone loss.
Alveolar ridge dimensional changes
Studies in this category confirmed that CBCT evaluation contributes to a better understanding of tissue biology and other changes to bone structure that occur after tooth extraction or bone grafting. Immediate implant placement, ridge preservation, volume stability during advanced grafting procedures of the maxillary sinus, and regenerative outcomes after flapless procedures are just a few of the treatments that benefit when CBCT is used to properly treatment plan the case.
Artifacts
No matter which imaging modality is used, the metallic nature of implants causes artifacts and interference that makes diagnosis difficult, with noise and beam-hardening being the most common issue for CBCT. Studies in this category concluded that advanced imaging software algorithms are required to decrease the implant-related beam-hardening artifacts on CBCT scans.14 Research on reducing artifacts caused by implants is ongoing.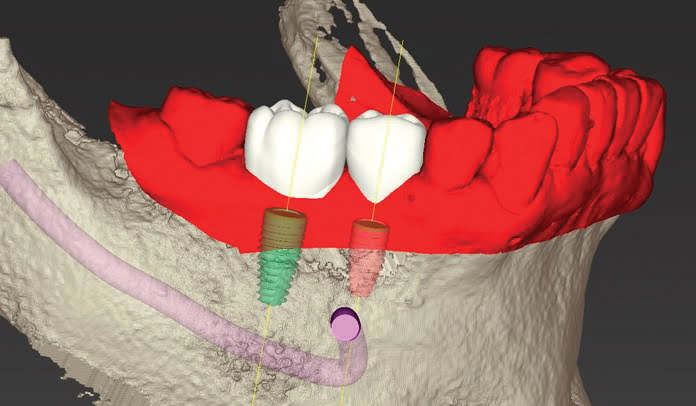 Figure 5: In this case, the DICOM data from the CS 9300 (tan) was merged with the .STL file generated from the CS 3600 intraoral scanner (red). Virtual crowns were created, and the implants were virtually placed as shown for fabrication of a restric-tive tooth-borne surgical guide to allow for guided implant surgery to be performed
Figure 5: In this case, the DICOM data from the CS 9300 (tan) was merged with the .STL file generated from the CS 3600 intraoral scanner (red). Virtual crowns were created, and the implants were virtually placed as shown for fabrication of a restric-tive tooth-borne surgical guide to allow for guided implant surgery to be performed
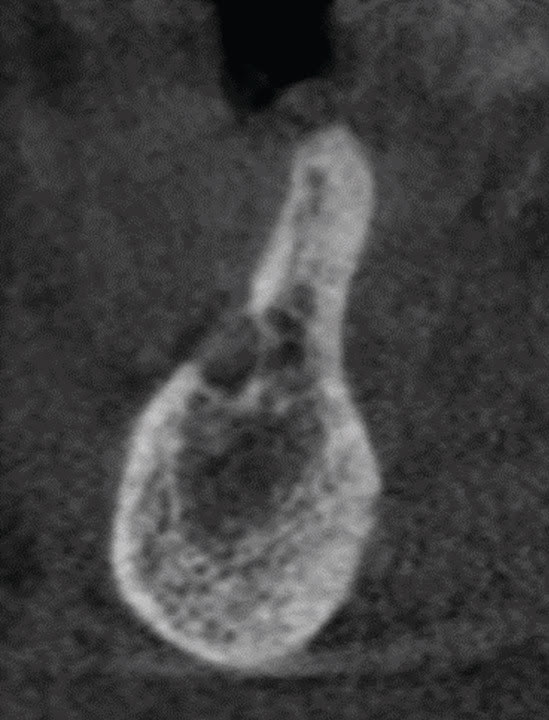 Figure 6: This CBCT scan of the posterior mandible shows the location of the mental foramen as well as how the region has limited vertical and horizontal bone.
Figure 6: This CBCT scan of the posterior mandible shows the location of the mental foramen as well as how the region has limited vertical and horizontal bone.  Bone grafting was performed with titanium mesh and a cellular allograft as shown in Figure 7. This CS 9300 CBCT system rendering shows the postoperative result following bone grafting of the case shown in Figure 6
Bone grafting was performed with titanium mesh and a cellular allograft as shown in Figure 7. This CS 9300 CBCT system rendering shows the postoperative result following bone grafting of the case shown in Figure 6
CBCT for implant treatment planning
Many studies focus on the different ways CBCT technology can be used for treatment planning. Both guided implant surgery and full navigational surgery have received a considerable amount of research validating their use.
Guided implant surgery
CBCT-driven implant treatment planning for guided implant surgery cannot be accomplished without third-party software. Importing DICOM files into third-party software for virtual planning and simulation before fabricating a restrictive surgical guide is an increasingly common form of CBCT-aided implant treatment planning. Virtual planning aids in determining the ideal location and angulation of the implant and allows clinicians to sometimes take a flapless approach. More and more, CBCT data is being paired with optical imaging data from intraoral scanners and combined with CAD/CAM technology to simultaneously plan the implant and the final restoration. This merger of data sets is an evolving technology that has been found to have great precision (Figure 5).
Surgical navigation systems are taking the CBCT-aided guided surgery to a new level. While the accuracy of this kind of surgery has been tested and looks promising, further research is needed. In comparison to both passive and active use of CBCT in preparation for surgery, studies found that freehand surgery was significantly less accurate.16
Accuracy of measurements
In regards to treatment planning, CBCT is seen to be particularly useful in measuring the height and width of the alveolar ridge. Measurements of bone quantity in the maxilla and mandible taken from a CBCT scan have also been found to be reliable.
Angular accuracy: Studies in this sub-category evaluated angular deviation after virtually planned surgery by comparing the virtual angle to the actual angle of the final implant. It was found there is less deviation when performing virtually planned surgery than compared to freehand surgery.16 Another study found that even less deviation exists between the virtual and the final angle of the implant when restrictive dental drill guides are used during surgery.
Linear accuracy: Linear measurements are more accurate when obtained with CBCT than 2D radiographs. Additionally, there is no significant difference in the linear measurements when using different field of views. Finally, studies in this sub-category found metallic artifacts don’t affect the accuracy of linear measurements taken with CBCT.16 Figure 8: This CBCT rendering shows the vertical fracture on tooth No. 29 with no buccal plate remaining and limited space to the mental foramen
Figure 8: This CBCT rendering shows the vertical fracture on tooth No. 29 with no buccal plate remaining and limited space to the mental foramen Figure 9: This CBCT-derived cross-sectional image of the case from Figure 8 clearly shows the mental foramen and how much bone is available to engage the planned immediate implant with substantial bone grafting
Figure 9: This CBCT-derived cross-sectional image of the case from Figure 8 clearly shows the mental foramen and how much bone is available to engage the planned immediate implant with substantial bone grafting Figure 10: This CBCT-derived cross-sectional image of the maxillary sinus shows a large blood vessel in close proximity to the proposed lateral window location. The window was placed inferior to the blood vessel to avoid bleeding and maintain ideal vascularization to the area during healing
Figure 10: This CBCT-derived cross-sectional image of the maxillary sinus shows a large blood vessel in close proximity to the proposed lateral window location. The window was placed inferior to the blood vessel to avoid bleeding and maintain ideal vascularization to the area during healing
CBCT for anatomical characterization
CBCT gives clinicians high-resolution, three-dimensional views of ridge topography and the location of critical anatomy to determine if advanced grafting procedures will be needed at the implant site (Figures 6-7). It’s been well established that 3D is superior to 2D imaging in this regard. CBCT studies on some of the relevant anatomy typically assessed during implant planning have been summarized below.
Neurovascular canal and foramina
CBCT can help clinicians avoid serious issues by clearly indentifying vital nerves and other anatomical structures that could be affected during implant surgery. Cross-sectional imaging makes it easier to identify neurovascular anatomical structures, such as the inferior alveolar nerve and the mental foramen (Figures 8-9), to name just a few. Manuscripts on nerve identification software reveal that imaging technology is under development that could be used to automatically identify the mandibular canal.18 CBCT imaging has also been found to be useful in locating large blood vessels in the lateral wall of the maxillary sinus, which can allow for improved window location during sinus augmentation procedures (Figure 10). During surgery, only 10% of “adverse events” occurred when preoperative CBCT images of the aforementioned anatomy had been taken, though that number jumped to 30%-50% when using other imaging modalities.19
Buccal/lingual bone
The thin facial bone plate on teeth is prone to resorption following extraction, which makes accurate measurements of the buccal and lingual plate vital prior to implant surgery (Figures 11-17). Studies have found CBCT imaging to be reliable in this area, and in fact, it is the only non-invasive means to evaluate the buccal and lingual plate.20 It should be noted that due to implant-related artifacts, CBCT accuracy in measuring the buccal plate tends to decrease during post-implant assessment of the buccal plate. However, studies have shown there are only minimal differences between CBCT measurements and histological measurements indicating that CBCT can be relied upon to provide useful measurements of bone levels on the buccal and lingual of implants.21
 Figure 11: This 2D radiograph of failed tooth No. 9 does not give much information to aid the surgeon in deciding on the flap design and determining if this case would be an appropriate case for an immediate implant with bone grafting and a provisional crown
Figure 11: This 2D radiograph of failed tooth No. 9 does not give much information to aid the surgeon in deciding on the flap design and determining if this case would be an appropriate case for an immediate implant with bone grafting and a provisional crown
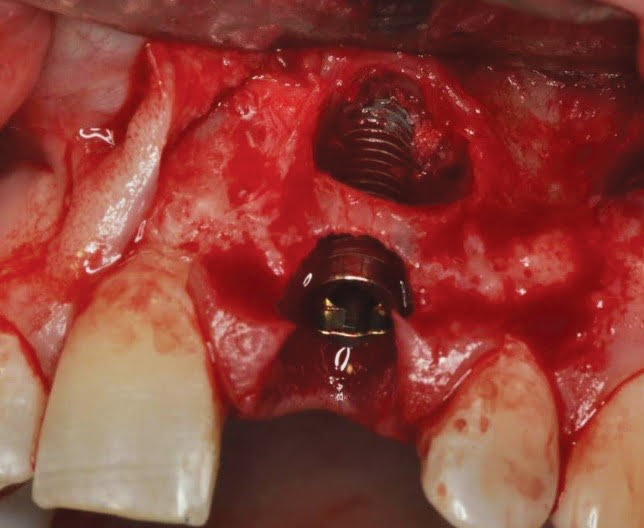 Figure 14: This clinical view shows the defect degranu-lated, the implant in place prior to bone graft placement, and provisional crown placement
Figure 14: This clinical view shows the defect degranu-lated, the implant in place prior to bone graft placement, and provisional crown placement
 Figure 12: The preoperative clinical view of the case in Figure 11, showing a high smile line
Figure 12: The preoperative clinical view of the case in Figure 11, showing a high smile line
 Figure 15: This CBCT-generated cross-sectional slice view was taken after 4 months of healing, just prior to the final restoration. The image shows the regenerated buccal bone exceeds 2 mm in dimension
Figure 15: This CBCT-generated cross-sectional slice view was taken after 4 months of healing, just prior to the final restoration. The image shows the regenerated buccal bone exceeds 2 mm in dimension
 Figure 17: This clinical view shows the final clinical result of the implant restored. Restorative procedures were completed by Thomas Orazio, DMD, utilizing Davis Dental Lab
Figure 17: This clinical view shows the final clinical result of the implant restored. Restorative procedures were completed by Thomas Orazio, DMD, utilizing Davis Dental Lab
 Figure 13: The CBCT scan shows much more information than the 2D radiograph — the significant periapical pathology and limited buccal plate. With this much destruction, a papilla-preserving flap was elevated to allow for complete defect degranulation and aggressive bone grafting
Figure 13: The CBCT scan shows much more information than the 2D radiograph — the significant periapical pathology and limited buccal plate. With this much destruction, a papilla-preserving flap was elevated to allow for complete defect degranulation and aggressive bone grafting
 Figure 16: This CBCT-generated axial slice view taken after 4 months of healing shows the ideal position of the implant shown in Figures 11-17. The implant is ideally placed relative to the adjacent teeth and the nasopalatine canal, with the ideal 2 mm of buccal bone for gingival stability
Figure 16: This CBCT-generated axial slice view taken after 4 months of healing shows the ideal position of the implant shown in Figures 11-17. The implant is ideally placed relative to the adjacent teeth and the nasopalatine canal, with the ideal 2 mm of buccal bone for gingival stability
Maxillary sinus
CBCT assessment of the maxillary sinuses prior to placing implants in the posterior maxilla has proven accurate in revealing anatomical and pathological variations. Particularly in regards to pre-sinus augmentation evaluation, studies confirm that CBCT is “significantly more reliable than panoramic imaging in detecting pathology and anatomic challenges”22 (Figures 18-21).
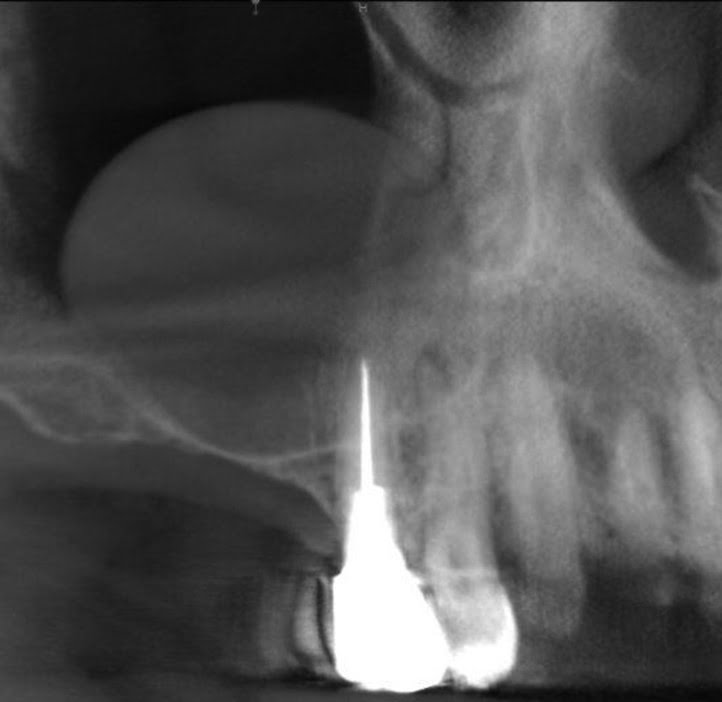 Figure 18: This preoperative CBCT panoramic image shows a mucous retention cyst in the maxillary sinus. Due to the large size of the cyst, sinus grafting is contraindicated until the cyst is treated
Figure 18: This preoperative CBCT panoramic image shows a mucous retention cyst in the maxillary sinus. Due to the large size of the cyst, sinus grafting is contraindicated until the cyst is treated
 Figure 19: This cross-sectional CBCT slice shows the extent of the cyst.
Figure 19: This cross-sectional CBCT slice shows the extent of the cyst.
 Figure 20: This cross-sectional CBCT slice verifies the elimination of the cyst following a small procedure performed 8 weeks prior to the sinus augmentation procedure
Figure 20: This cross-sectional CBCT slice verifies the elimination of the cyst following a small procedure performed 8 weeks prior to the sinus augmentation procedure
 Figure 21: This preoperative CBCT generated axial slice view shows multiple septa in the maxillary sinus, which will significantly complicate the sinus augmentation procedure
Figure 21: This preoperative CBCT generated axial slice view shows multiple septa in the maxillary sinus, which will significantly complicate the sinus augmentation procedure
Bone density
CBCT’s use for evaluating bone density is an increasing area of interest. Due to the technology that powers the modality — acquisition algorithms, reconstruction of data sets, etc. — Hounsfield units and linear attenuation coefficients are not as easy to calculate with CBCT as medical CT. As of now, only relative bone quality can be assessed using CBCT. However, efforts are currently underway to standardize imaging variables to confirm the reliability of bone density measurements taken with CBCT. In the meantime, studies show that quantitative CBCT (QCBCT) may serve as an alternative tool for evaluating bone density prior to surgery.23
Conclusion
The consensus concludes: “CBCT is a useful and widely available tool in implant dentistry that has the potential to improve today’s standard of care.” The valuable 3D views CBCT provides can significantly change the course of treatment. Additionally, new imaging software is rapidly enhancing the use of CBCT, making it more intuitive and a better tool for virtual treatment planning. As an added benefit, the digital file format of CBCT scans is easily transferable when working with referrals.
Research is ongoing in implant dentistry to demonstrate the value of CBCT, though it’s irrefutable that 3D imaging is supplanting traditional radiographic methods. The wealth of literature evaluated and the expert opinion generated during the BEC meeting will allow the AAP to continue to provide guidance for its members on CBCT use. This has been a brief review of some of the key findings from the conference, and the full consensus publications are now available in the Journal of Periodontology. These papers should be considered a must-read for those involved in implant dentistry and for all clinicians using CBCT technology.
Author Info
 Bradley S. McAllister, DDS, PhD, obtained his doctorate of dental surgery at the University of Washington. He then attended the University of Texas Health Science Center at San Antonio where he completed his residency in periodontics and earned his PhD. His ongoing research has been focused on techniques to improve surgical wound healing with growth factors and stem cell therapy. For more than 20 years, he’s practiced periodontology in Portland, Oregon, and currently serves as faculty in Oregon Health and Science University’s Department of Periodontology. Dr. McAllister serves on the American Academy of Periodontology scientific oversight committee and is chair of its Best Evidence Consensus advisory working group
Bradley S. McAllister, DDS, PhD, obtained his doctorate of dental surgery at the University of Washington. He then attended the University of Texas Health Science Center at San Antonio where he completed his residency in periodontics and earned his PhD. His ongoing research has been focused on techniques to improve surgical wound healing with growth factors and stem cell therapy. For more than 20 years, he’s practiced periodontology in Portland, Oregon, and currently serves as faculty in Oregon Health and Science University’s Department of Periodontology. Dr. McAllister serves on the American Academy of Periodontology scientific oversight committee and is chair of its Best Evidence Consensus advisory working group
 V. Thomas Eshraghi, DMD, completed both his periodontal specialty training and dental school at the Oregon Health and Science University. As an assistant professor, he also trains residents in Oregon Health and Science University’s periodontics graduate program. His active research is in the area of stem cell technology. Dr. Eshraghi actively lectures on periodontics, implantology and the incorporation of advanced digital technologies in the treatment of periodontal disease.
V. Thomas Eshraghi, DMD, completed both his periodontal specialty training and dental school at the Oregon Health and Science University. As an assistant professor, he also trains residents in Oregon Health and Science University’s periodontics graduate program. His active research is in the area of stem cell technology. Dr. Eshraghi actively lectures on periodontics, implantology and the incorporation of advanced digital technologies in the treatment of periodontal disease. Hector F. Rios, DDS, PhD, is an adjunct clinical associate professor in the Department of Periodontics and Oral Medicine at the University of Michigan. Dr. Rios received his dental degree at the University of Valle, Cali-Colombia. He completed his periodontics residency at the University of Michigan and earned an interdisciplinary PhD in oral biology and molecular biology at the University of Missouri-Kansas City. He is a Diplomate of American Board of Periodontology and maintains a private practice limited to periodontics and dental implants in Holland, Michigan.
Hector F. Rios, DDS, PhD, is an adjunct clinical associate professor in the Department of Periodontics and Oral Medicine at the University of Michigan. Dr. Rios received his dental degree at the University of Valle, Cali-Colombia. He completed his periodontics residency at the University of Michigan and earned an interdisciplinary PhD in oral biology and molecular biology at the University of Missouri-Kansas City. He is a Diplomate of American Board of Periodontology and maintains a private practice limited to periodontics and dental implants in Holland, Michigan.Disclosure: Dr. McAllister is one of Carestream Dental’s key opinion leaders.
References
- Rios HF, Borgnakke WS, Benavides E. The use of cone-beam computed tomography in the management of the patient requiring dental implants: An American Academy of Periodontology best-evidence review. J Periodontol. 2017;88:946-959.
- Kim DM, Bassir SH. When is cone-beam computed tomography imaging appropriate for diagnostic inquiry in the management of inflammatory periodontitis? An American Academy of Periodontology best-evidence review. J
Periodontol. 2017;88:978-998. - Mandelaris GA, Neiva R, Chambrone L. Cone-beam computed tomography and interdisciplinary dentofacial therapy: An American Academy of Periodontology best-evidence review focusing on risk assessment of the dento-alveolar bone changes influenced by tooth movement. J Periodontol. 2017;88:960-977.
- Mandelaris GA, Scheyer ET, Evans M, Kim DM, McAllister B, Nevins ML, Rios HF, Sarment D. American Academy of Periodontology’s best-evidence consensus statement on selected oral applications for cone-beam computed tomography. J Periodontol. 2017;88:939-945.
- American Association of Endodontics and American Academy of Oral and Maxillofacial Radiology. AAE and AAOMR Joint Position Statement. Use of Cone Beam Computed Tomography in Endodontics 2015 Update. 2016; Special Committee to Revise the AAE/AAOMR Joint Position Statement on Cone Beam Computed Tomography. https://www.aae.org/uploadedfiles/clinical_resources/guidelines_and_position_statements/cbctstatement_2015update.pdf.
- Eshraghi T, McAllister N, McAllister B. Clinical applications of digital 2-D and 3-D radiography for the periodontist. J Evid Base Dent Pract. 2012;12(suppl 3):36-45
- Price JB, Thaw KL, Tyndall DA, Ludlow JB, Padilla RJ. Incidental findings from cone beam computed tomography of the maxillofacial region: a descriptive retrospective study. Clin Oral Implants Res. 2012;23(11):1261-1268.
- Mandian M, Tadinada A. Incidental findings in the neck region of dental implant patients: a comparison between panoramic radiography and CBCT. J Mass Dent Soc. 2014;63(2):42-45.
- Kaeppler G, Mast M. Indications for cone-beam computed tomography in the area of oral and maxillofacial surgery. Int J Comput Dent. 2012;15(4):271-286.
- Pette GA, Norkin FJ, Ganeles J, et al. Incidental findings from a retrospective study of 318 cone beam computed tomography consultation reports. Int J Oral Maxillofac Implants. 2012;27(3):595-603.
- Barghan S, Tetradis S, Nervina JM. Skeletal and soft-tissue incidental findings on cone-beam computed tomography images. Am J Orthod Dentofacial Orthop. 2013;143(6):888-892.
- Allareddy V, Vincent SD, Hellstein JW, Qian F, Smoker WR, Ruprecht A. Incidental findings on cone beam computed tomography images. Int J Dent. 2012;2012:871532. doi:10.1155/2012/871532.
- Malloy K, Wadhwani C, McAllister B, Wang M, Katancik J. Accuracy and reproducibility of radiographic images for assessing crestal bone height of implants using the precision implant X-ray locator (PIXRL) device. Int J Oral Maxillofac Implants. 2017;32(4):830-836.
- Naitoh M, Nabeshima H, Hayashi H, et al. Postoperative assessment of incisor dental implants using cone-beam computed tomography. J Oral Implantol. 2010;36(5):377-384.
- Pauwels R, Stamatakis H, Bosmans H, et al. Quantification of metal artifacts on cone beam computed tomography images. Clin Oral Implants Res 2013;24 (suppl A 100):94-99.
- Vermeulen J. The accuracy of implant placement by experienced surgeons: guided vs freehand approach in a simulated plastic model. Int J Oral Maxillofac Implants. 2017;32(3):617-624.
- Cremonini CC, Dumas M, Pannuti CM, Neto JB, Cavalcanti MG, Lima LA.. Assessment of linear measurements of bone for implant sites in the presence of metallic artifacts using cone beam computed tomography and multislice computed tomography. Int J Oral Maxillofac Surg. 2011;40(8):845-850.
- Abdolali F, Zoroofi RA, Abdolali M, Yokota F, Otake Y, Sato Y. Automatic segmentation of mandibular canal in cone beam CT images using conditional statistical shape model and fast marching. Int J Comput Assist Radiol Surg. 2017;12:581-593.
- Benavides E, Rios HF, Ganz SD, et al. Use of cone beam computed tomography in implant dentistry: the International Congress of Oral Implantologists consensus report. Implant Dent. 2012;21(2):78-86.
- Miyamoto Y, et al. Analyses of PO Buccal Bone Thickness in Maxillary Anterior Implants. J Perio Rest Dent. CTBC
- Huang Y, Van Dessel J, Depypere M, et al. Validating cone-beam computed tomography for peri-implant bone morphometric analysis. Bone Res. 2014;2:14010.
- Tadinada A, Jalali E, Al-Salman W, Jambhekar S, Katechia B, Almas K. Prevalence of bony septa, antral pathology, and dimensions of the maxillary sinus from a sinus augmentation perspective: a retrospective cone-beam computed tomography study. Imaging Sci Dent. 2016;46(2):109-115.
- Aranyarachkul P, Caruso J, Gantes B, et al. Bone density assessments of dental implant sites; 2. quantitative cone-beam computerized tomography. Int J Oral Maxillofac Implants. 2005;20(3):416-424.
Stay Relevant With Implant Practice US
Join our email list for CE courses and webinars, articles and mores
