Educational aims and objectives
This self-instructional course for dentists discusses innovative methods for utilizing intraoral scanners to capture full-arch implant positioning for a fully digital All-on-X workflow.
Expected outcomes
Implant Practice US subscribers can answer the CE questions by taking the quiz online to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
- Identify several methods for digitally recording implant positioning.
- Realize some factors that can influence the accuracy of the scans.
- Identify the process of grammetry.
- Observe two Scanbase tracking systems used by the author to facilitate a fully digital workflow for full-arch implant cases.
Dr. Christopher R. Resnik educates readers on intraoral scanning and its role in All-on-X implant-supported reconstructions.
Dr. Christopher R. Resnik discusses some advances in intraoral scanning devices and acquisition technology
All-on-X implant-supported reconstructions provide an excellent opportunity to restore the function of the dental arch, while improving the quality of lives of our patients. Innovations on the surgical and restorative fronts are evolving at an accelerated rate, facilitating faster, more accurate workflows and results. As the dental industry continues to strive for fully digital solutions, advances in intraoral scanning devices and acquisition technology are widening the disparity between digital and analog methods, favoring intraoral scanning (IOS) as a more viable solution. However, when treating fully edentulous implant cases, there are still inherent inaccuracies associated with conventional intraoral scanning.1
Photogrammetry, at this time, remains the sole validated and most accurate method for digitally recording implant positioning.2 However, drawbacks to photogrammetry include high cost, limited applicability (i.e., full-arch implant impressions), and high demand. Fewer dental offices, therefore, possess photogrammetry units, while many dental offices have access to intraoral scanners. Innovative methods have therefore been developed utilizing intraoral scanners to capture full-arch implant positioning for a fully digital All-on-X workflow.
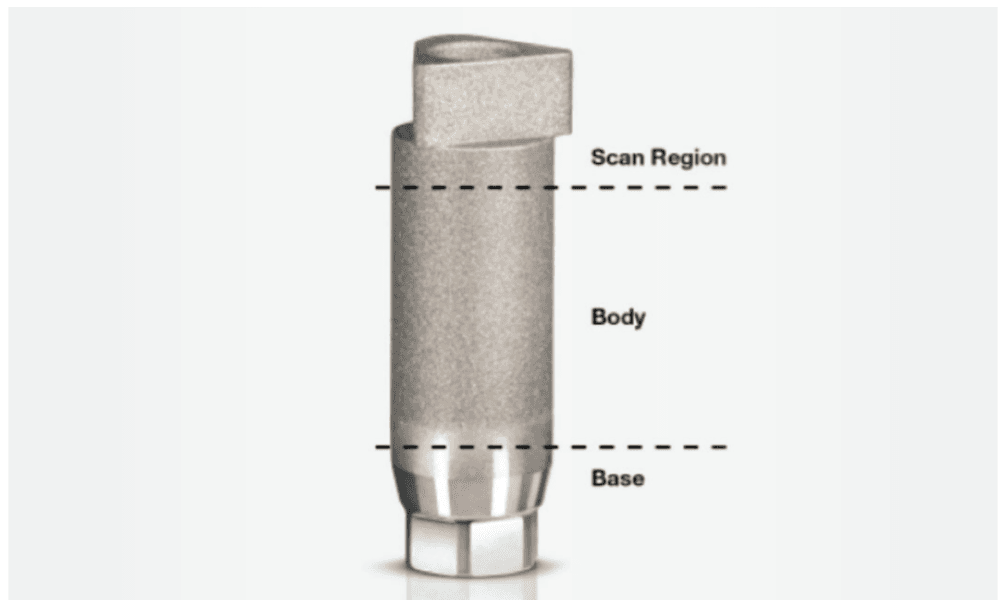
Intraoral scanners create a 3D virtual model of dentition, soft tissue, and implant position by compiling multiple individual images that are created from a beam of light. For digital implant impressions, a “scan body” is inserted into the dental implant and scanned circumferentially. A virtual model is created, converted to a stereolithography (STL) file, imported into design software, and a restoration is designed. Traditional scan bodies are vertical, with the top one-third of the scan body, termed the “scan region,” being the critical part that must be recorded accurately (Figure 1). Studies have found that for single and multiple implants, intraoral scanning is as accurate or even more accurate than traditional analog impressions.3,4 However, when obtaining full-arch scans, there are several inherent factors that influence the accuracy of the scan.
- Environmental and intraoral factors: Blood, saliva, and soft tissue (i.e., tongue) create complications and inaccuracies with IOS. Soft tissues can move or deform during scanning, leading to inaccuracies in the final impression.5
- Patient factors: Accessibility of the intraoral scanner tip is influenced by its size, the implant location, and the patient’s ability to open. Patient movement also impacts scan accuracy. Full-arch scans take longer to complete, increasing the likelihood of patient movement.
- Large scan area: Full-arch impressions require scanning a larger surface area compared to single site or partial-arch impressions. Maintaining accuracy over a larger surface is inherently more difficult. Errors can be attributed to the small wand size necessitating subsequent stitching of the fields together and the lack of significant landmarks between scan bodies. Small errors can accumulate over the length of the arch, leading to significant discrepancies in the final digital impression.6
- Multiple, varying implant angulations: The varying angles and positions of multiple implants can complicate the scanning process. Inconsistencies in capturing the exact orientation and position of each implant can lead to inaccuracies in the final impression.7 Some studies have evaluated the number of implants and found greater accuracy with fewer implants.8
- Scan body design: The scan body design, shape, material, and alignment influence the outcome of correct acquisition of implant positions.9,10
- Operator experience: The skill level of the operator significantly impacts the accuracy of IOS. Inexperienced operators may struggle with maintaining consistent scanning techniques, leading to errors.11,12 However, even experienced operators can face challenges with full arch scans due to the increased complexity.
- Scanning strategy: The pattern and method of scanning (e.g., segmental versus continuous) can influence the precision and trueness of digital impressions. Different scanning strategies may yield varying levels of accuracy, particularly in complex full-arch cases.13,14
- Scanner limitations: IOS systems have varying capabilities and limitations. Some scanners may perform well in capturing detailed images of smaller areas but may not be as effective for full arch impressions.15 Factors such as the type of scanning technology and the specific algorithms used by the scanner can affect the accuracy and reliability of the impressions.16
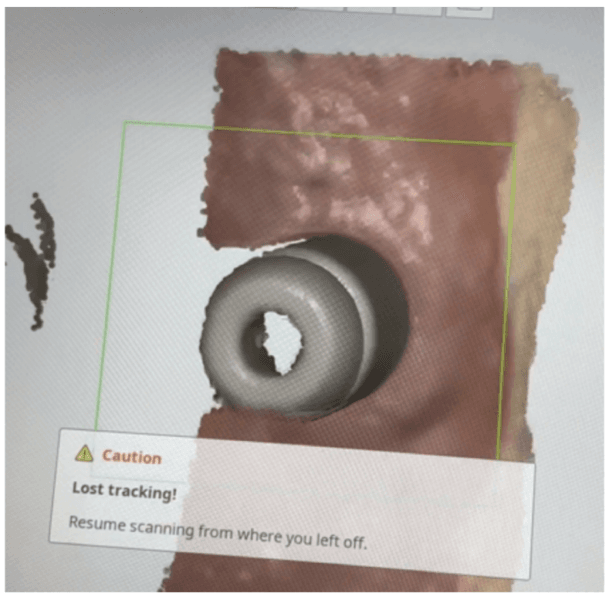
- Stitching errors: Intraoral scanners only capture a limited area at one time. The final model is generated by stitching images together. For completely edentulous scans, the lack of landmarks, long span of mobile mucosa, and multiple scan bodies may cause the images to be stitched incorrectly and lead to higher deviations9,16 (Figure 2). This is apparent as studies have found increased error with increased interimplant distance.17
Grammetry
Innovative techniques and scan bodies have been developed to help navigate the large scan areas and stitching inaccuracies involved with traditional, vertical independent scan bodies. Several techniques have been proposed to improve the full-arch digital implant impression accuracy such as the use of fiducial markers,18 auxiliary clips,19 splinting scan bodies together,20 interim prostheses,21 pressure-indicating paste,22 auxiliary geometric appliances,23 and scan powder.24
Grammetry is a method developed that rivals photogrammetry and analog implant impression techniques. Grammetry is the process of capturing a continuous arch scan with an intraoral scanner and a unique ScanBase tracking mechanism, preventing loss of accuracy ensuring scan quality. Utilizing a special Scanbase system, the scan bodies are connected together allowing for a continuous scan with the intraoral scanner, decreasing the chance of stitching errors. Described below are two Scanbase tracking systems that are utilized by the author in private practice. Both techniques provide simplified scanning, improved accuracy, and a fully digital workflow for full-arch implant cases.
OPTISPLINT®
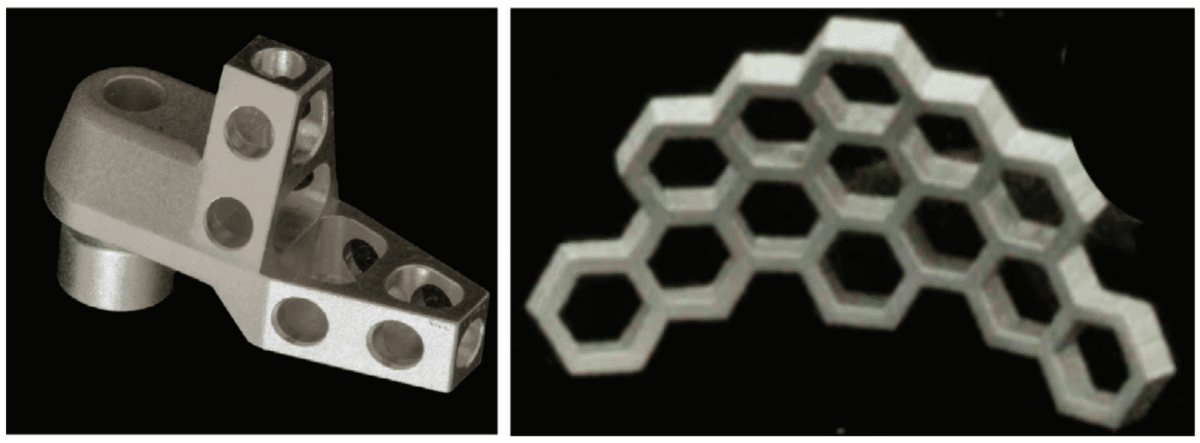
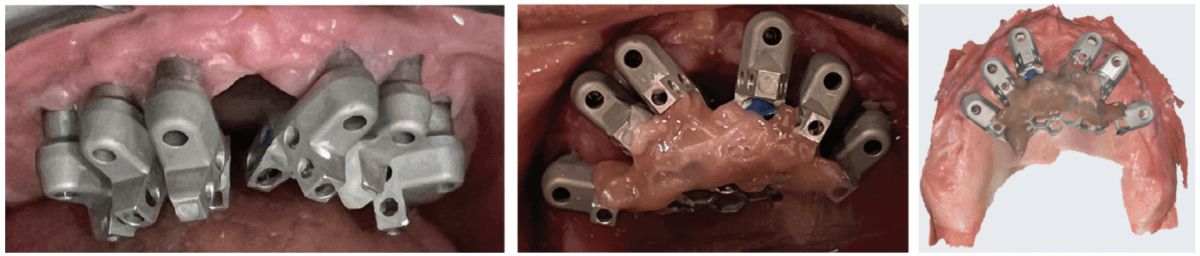
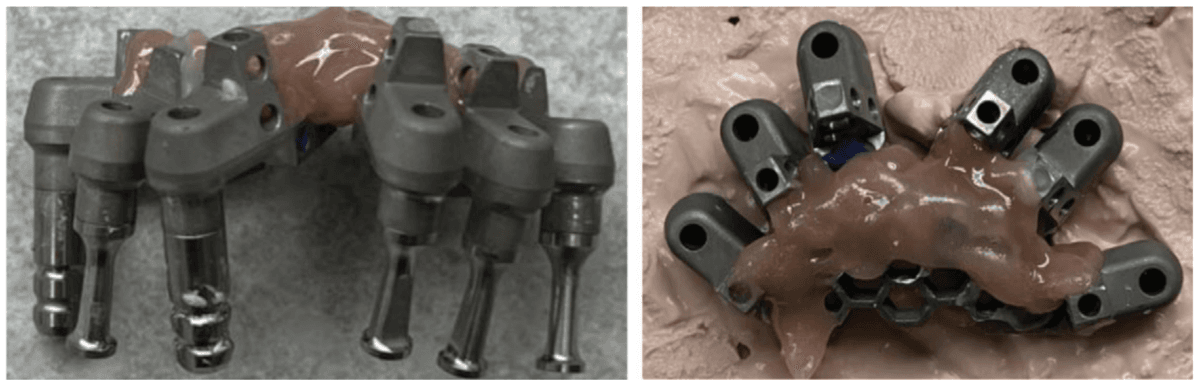
OPTISPLINT, by Digital Arches (https://digitalarches.com), is a dual-purpose implant coping, which serves as an abutment level scan body for fixed complete-arch prostheses as well as an analog verification jig. Individual scan bodies are inserted on each multi-unit abutment individually (Figure 4A). This scan body is unlike a traditional scan body, where a wing-like extension is cantilevered off of the scan region (Figure 3A). A central honeycomb metal frame piece is then placed, adjusted if necessary, within 1 mm-2 mm of wing components of the scan body (Figure 3B). Resin (flowable composite, dual-polymerizing, auto-polymerizing) or acrylic is then added to lute the scan bodies to the central honeycomb metal frame piece (Figure 4B). Once all scan bodies are attached, the OPTISPLINT jig can then be scanned as a single, splinted object, intraorally or extraorally (Figure 4C). If completed extraorally, the patient’s factors (blood, saliva, soft tissue, limited opening) are eliminated. An added benefit of this system is that the OPTISPLINT jig can then be poured in dental stone to facilitate the fabrication of an accurate master cast (Figures 5A and 5B). This is beneficial for checking the passivity of the prosthesis prior to inserting and can aid with the cementation of ti-bases to the interim or final prosthesis.
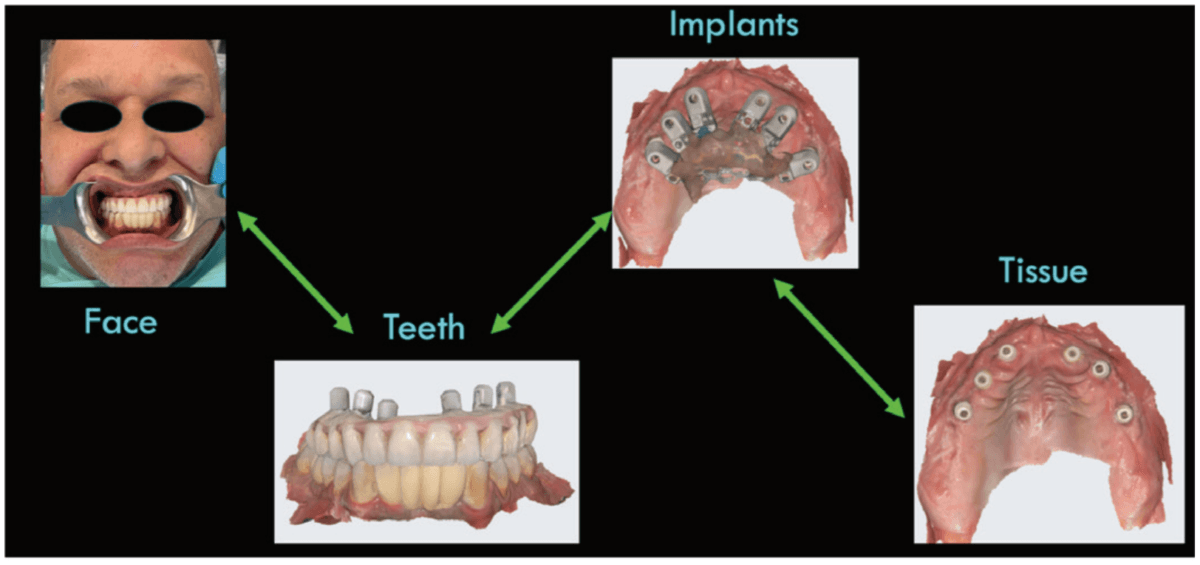
When imported into a design software (e.g., Exocad), the OPTISPLINT scan will produce a digital file of implant positioning. Additional records include facial records, soft tissue records, and tooth/occlusal records (Figure 6).
After all the records are acquired, the scans may then be aligned and the patient’s implant prosthesis can be designed and fabricated (Figures 7A-7F). The OPTISPLINT technique enables clinicians to utilize a fully-digital workflow for a fraction of the cost of other digital methods. Patient factors are able to be eliminated as the OPTISPLINT can be scanned extraorally with the added benefit of acting as a verification jig prior to prosthetic delivery.

CONnX Scan System
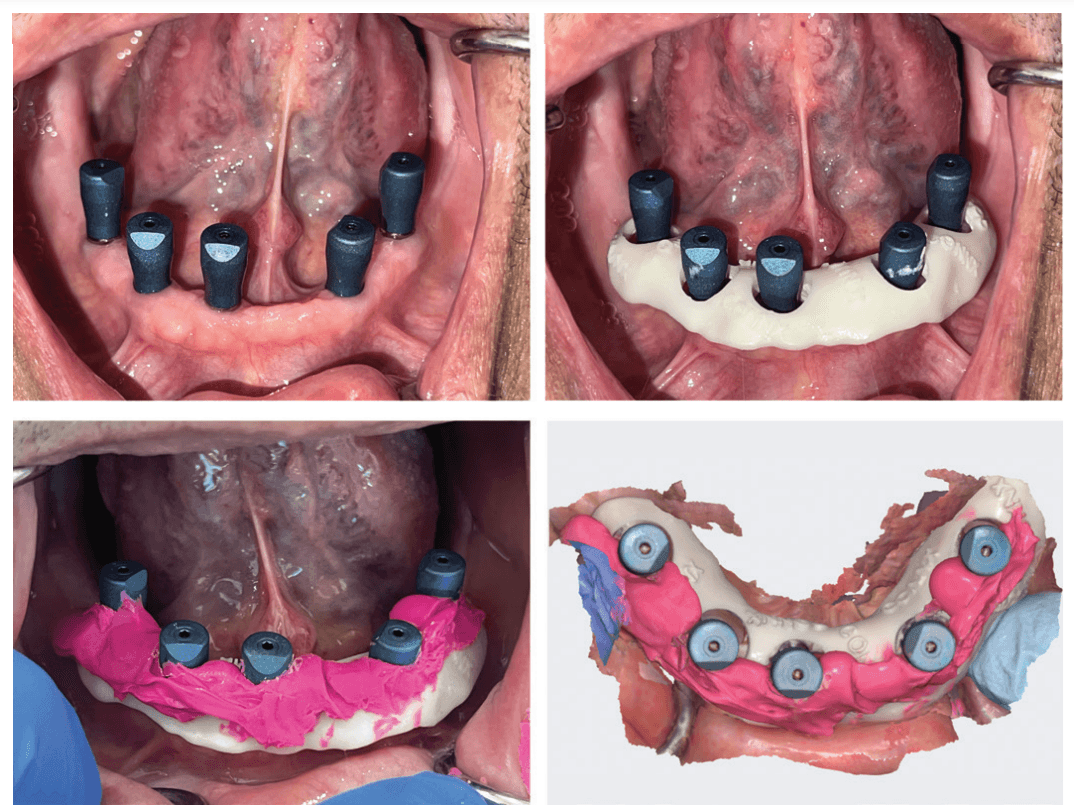
Another type of grammetry method is the CONnX Scan system, by Synergy Dental Lab (https://www.synrglab.com/). The CONnX Scan system utilizes individual scan bodies and connects them together with a tracking material. Individual scan bodies are available in different sizes (5 mm, 10 mm,15 mm depending on the height of the gingival tissue) and with a reverse scan body analog that can be inserted into a prosthesis (Figure 8). Individual scan bodies are placed on the multi-unit abutments, then through two different methods, are connected together allowing for a continuous scan. One method involves placing ScanLink (Rigid Bite Registration Material) around the scan bodies to connect them together, leaving 5 mm of the scan body exposed to allow capturing of the scan region (Figures 9A-9D). The ScanLink allows the intraoral scanner to capture the scan regions continuously. The second method involves placement of a ScanBase around the scan bodies. The ScanBase is a printed composite material that is custom made for each patient (Figure 10). Specific geometrical shapes are present on the ScanBase which allow the intraoral scanner to pick up details that aid in stitching. If needed, ScanLink may also be added to the ScanBase to allow for easier scanning.


By connecting the scan bodies together with the CONnX Scan system, the area the scanner needs to travel between the scan regions of neighboring scan bodies is decreased, thereby improving accuracy and stitching capability. The final digital file of the intraoral scan will then be uploaded into the CAD software. Similar digital records also acquired include facial records, soft tissue records, and tooth/occlusal records.
All of the digital files are then exported to the dental lab for fabrication of the full-arch implant prosthesis, utilizing a fully digital workflow (Figures 11A-11D). ScanLink and ScanBase allow the intraoral scanner to capture the scan regions more accurately, with less stitching errors compiling the various images. The option for multiple sizes of scan bodies with the same scan region accompanied with a reverse scan analog allows easier alignment of digital data and a smoother transition to the prosthetic manufacturing.

“Grammetry, through utilization of a scan base system, allows the intraoral scanner to continuously capture data which has led to improved accuracy in full-arch digital implant impressions.”
Summary
While intraoral scanning offers many advantages, such as patient comfort and digital integration, it faces significant challenges when utilized in full-arch implant impressions. The large surface area in edentulous cases, lack of stable reference points, lack of teeth or keratinized mucosa, and the similarities in scan body morphology make it difficult to distinguish and stitch together multiple images accurately. Innovative scanning techniques and scan body systems have strived to overcome these challenges. Grammetry, through utilization of a scan base system, allows the intraoral scanner to continuously capture data which has led to improved accuracy in full-arch digital implant impressions. OPTISPLINT and the CONnX Scan system are two types of these scan base systems that connect the scan bodies together, thus limiting stitching difficulties. With these techniques, the everyday clinician is able to utilize their intraoral scanner for a fully digital All-on-X workflow.
We are at a time in implant dentistry of rapidly evolving products, techniques, and workflows. The Resnik Implant Institute has implemented these digital methods into their surgical, prosthetic, and hands-on curriculums. Attendees receive didactic and hands-on training with photogrammetry, intraoral scanning techniques, and alignment of all data to allow for the ultimate experience in prosthetic digital designs. Teaching these contemporary methods, as well as the foundation of implant dentistry, helps doctors understand and appropriately implement these updated technologies and workflows into their practices.
Read how intraoral scanning is an important part of the digital implant planning process, and how this scanner is part of a faster and more powerful generation of scanners. https://implantpracticeus.com/industry-news/cs-3700-intraoral-scanner-ranked-high-for-reliability-when-scanning-implants-study-shows/
Author Info
 Christopher R. Resnik, DMD, MDS, DICOI, is a prosthodontist in private practice in Winter Park, Florida. He completed his dental degree, prosthodontic residency, and master’s degree in oral implantology from the University of Pittsburgh School of Dental Medicine. Dr. Resnik holds associate faculty positions at the University of Pittsburgh Graduate Prosthodontic Program and Temple University Graduate Periodontics Program. He is a contributing author to multiple textbooks including Avoiding Complications in Oral Implantology, Misch’s Contemporary Implant Dentistry, and Dental Implant Prosthetics.
Christopher R. Resnik, DMD, MDS, DICOI, is a prosthodontist in private practice in Winter Park, Florida. He completed his dental degree, prosthodontic residency, and master’s degree in oral implantology from the University of Pittsburgh School of Dental Medicine. Dr. Resnik holds associate faculty positions at the University of Pittsburgh Graduate Prosthodontic Program and Temple University Graduate Periodontics Program. He is a contributing author to multiple textbooks including Avoiding Complications in Oral Implantology, Misch’s Contemporary Implant Dentistry, and Dental Implant Prosthetics.
Disclosure: Dr. Resnik is a faculty member of the Resnik Implant Institute. He reports no other conflicts of interests with the companies mentioned in this article.
References
- Kim KR, Seo KY, Kim S. Conventional open-tray impression versus intraoral digital scan for implant-level complete-arch impression. J Prosthet Dent. 2019 Dec;122(6): 543-549.
- Resnik C. The use of photogrammetry for the fabrication of full-arch immediate prostheses. Implant Practice US. Fall 2023;16(3):26-30.
- Albanchez-González MI, Brinkmann JC, Peláez-Rico J, López-Suárez C, Rodríguez-Alonso V, Suárez-García MJ. Accuracy of Digital Dental Implants Impression Taking with Intraoral Scanners Compared with Conventional Impression Techniques: A Systematic Review of In Vitro Studies. Int J Environ Res Public Health. 2022 Feb 11;19(4):2026.
- Schmidt A, Wöstmann B, Schlenz MA. Accuracy of digital implant impressions in clinical studies: A systematic review. Clin Oral Implants Res. 2022 Jun;33(6):573-585.
- Mangano FG, Admakin O, Bonacina M, Lerner H, Rutkunas V, Mangano C. Trueness of 12 intraoral scanners in the full-arch implant impression: a comparative in vitro study. BMC Oral Health. 2020 Sep 22;20(1):263.
- Gehrke P, Rashidpour M, Sader R, Weigl P. A systematic review of factors impacting intraoral scanning accuracy in implant dentistry with emphasis on scan bodies. Int J Implant Dent. 2024 May 1;10(1):20.
- van der Meer WJ, Andriessen FS, Wismeijer D, Ren Y. Application of intra-oral dental scanners in the digital workflow of implantology. PLoS One. 2012;7(8):e43312.
- Gherlone EF, Ferrini F, Crespi R, Gastaldi G, Capparé P. Digital impressions for fabrication of definitive “all-on-four” restorations. Implant Dent. 2015 Feb;24(1):125-129.
- Meneghetti PC, Li J, Borella PS, Mendonça G, Burnett LH Jr. Influence of scanbody design and intraoral scanner on the trueness of complete arch implant digital impressions: An in vitro study. PLoS One. 2023 Dec 19;18(12):e0295790.
- Mizumoto RM, Yilmaz B. Intraoral scan bodies in implant dentistry: A systematic review. J Prosthet Dent. 2018 Sep;120(3):343-352.
- Pesce P, Bagnasco F, Pancini N, Colombo M, Canullo L, Pera F, Bressan E, Annunziata M, Menini M. Trueness of Intraoral Scanners in Implant-Supported Rehabilitations: An In Vitro Analysis on the Effect of Operators’ Experience and Implant Number. J Clin Med. 2021 Dec 16;10(24):5917.
- Flügge T, van der Meer WJ, Gonzalez BG, Vach K, Wismeijer D, Wang P. The accuracy of different dental impression techniques for implant-supported dental prostheses: A systematic review and meta-analysis. Clin Oral Implants Res. 2018 Oct;29 Suppl 16:374-392.
- Hardan L, Bourgi R, Lukomska-Szymanska M, Hernández-Cabanillas JC, Zamarripa-Calderón JE, Jorquera G, Ghishan S, Cuevas-Suárez CE. Effect of scanning strategies on the accuracy of digital intraoral scanners: a meta-analysis of in vitro studies. J Adv Prosthodont. 2023 Dec;15(6):315-332.
- Ma J, Zhang B, Song H, Wu D, Song T. Accuracy of digital implant impressions obtained using intraoral scanners: a systematic review and meta-analysis of in vivo studies. Int J Implant Dent. 2023 Dec 6;9(1):48.
- Di Fiore A, Graiff L, Savio G, Granata S, Basilicata M, Bollero P, Meneghello R. Investigation of the Accuracy of Four Intraoral Scanners in Mandibular Full-Arch Digital Implant Impression: A Comparative In Vitro Study. Int J Environ Res Public Health. 2022 Apr 13;19(8):4719.
- Zhang YJ, Shi JY, Qian SJ, Qiao SC, Lai HC. Accuracy of full-arch digital implant impressions taken using intraoral scanners and related variables: A systematic review. Int J Oral Implantol (Berl). 2021 May 12;14(2):157-179.
- Di Fiore A, Meneghello R, Graiff L, Savio G, Vigolo P, Monaco C, Stellini E. Full arch digital scanning systems performances for implant-supported fixed dental prostheses: a comparative study of 8 intraoral scanners. J Prosthodont Res. 2019 Oct;63(4):396-403.
- Saaedi TMASE, Thabet YG. Customized scan bodies to facilitate intraoral scanning for full arch implant prosthesis: A dental technique. J Prosthodont. 2024 Mar;33(3):
297-300. - Etxaniz O, Amezua X, Jauregi M, Solaberrieta E. Improving the accuracy of complete arch implant digital scans by using auxiliary clips for intraoral scan bodies: A dental technique. J Prosthet Dent. 2024 Feb 27:S0022-3913(24)00066-0.
- Retana L, Nejat AH, Pozzi A. Effect of splinting scan bodies on trueness of complete-arch implant impression using different intraoral scanners: an in vitro study. Int J Comput Dent. 2023 Feb 24;26(1):19-28.
- Papaspyridakos P, Bedrossian A, Kudara Y, Ntovas P, Bokhary A, Chochlidakis K. Reverse scan body: A complete digital workflow for prosthesis prototype fabrication. J Prosthodont. 2023 Jun;32(5):452-457.
- Mizumoto RM, Yilmaz B, McGlumphy EA Jr, Seidt J, Johnston WM. Accuracy of different digital scanning techniques and scan bodies for complete-arch implant-supported prostheses. J Prosthet Dent. 2020 Jan;123(1):96-104.
- Iturrate M, Eguiraun H, Solaberrieta E. Accuracy of digital impressions for implant-supported complete-arch prosthesis, using an auxiliary geometry part-An in vitro study. Clin Oral Implants Res. 2019 Dec;30(12):1250-1258.
- Donmez MB, Çakmak G, Dede DÖ, Küçükekenci AS, Lu WE, Schumacher FL, Revilla-León M, Yilmaz B. Effect of scan powder and scanning technology on measured deviations of complete-arch implant supported frameworks digitized with industrial and intraoral scanners. J Dent. 2023 Nov;138:104736.
Stay Relevant With Implant Practice US
Join our email list for CE courses and webinars, articles and mores

