Educational aims and objectives
This article aims to describe the complex restorative and placement procedure required in a case resulting from major facial trauma.
Expected outcomes
Implant Practice US subscribers can answer the CE questions by taking the quiz to earn 2 hours of CE from reading this article.
Take the quiz by clicking here.
Correctly answering the questions will demonstrate the reader can:
- Identify surgical protocols applied in this case.
- Identify the characteristics and causes of penetrating injuries in the maxillofacial region.
- Recognize the phases to treatment planning a case such as this.
- Realize some statistics related to traumatic injuries as a result of work-related injuries.
- Recognize autogenous onlay block grafting from intraoral sites as a predictable treatment modality for reconstruction of large volume alveolar bone defects.
Drs. Muhammed Abram and André van Zyl describe treatment for dental injuries from an angle grinder using complex tissue regeneration.
Drs. Muhammed H. Abram and André van Zyl describe a case whereby one patient required complex tissue regeneration following a grinding disc injury.
Injuries to the maxillofacial region resulting from the use of angle grinders are often disfiguring. They can negatively influence phonetics and masticatory function as well as self-esteem. This article presents a case report wherein autogenous bone blocks followed by dental implant placement were used to reconstruct a large volume hard tissue defect caused by a grinding disc injury.
Introduction
Penetrating injuries are those that violate the soft and hard tissues by an object that forcefully enters the body. In the maxillofacial region, these injuries may either be isolated or any combination of contusions, abrasions, lacerations, dentoalveolar fractures, luxations in their several forms (lateral, intrusive, extrusive), subluxations, dental tissue lesions, and avulsions (Rodriguez and Guerrero, 2010; Koyuturk and Kusgoz, 2008).

In their study, Bastone, et al. (2000), found that males experienced significantly more facial trauma than females with male:female ratios ranging from 1.3-2.3:1. Most traumatic dental injuries are unintentional with the most dominating causes being falls, collisions, and being struck by an object (Glendor, 2009).
This article presents an unusual case of reconstruction of the dentoalveolar structures, carried out one year after an injury caused by a broken disc from an angle grinder.
Case report
A 35-year-old male presented to the Department of Periodontics and Oral Medicine, University of Pretoria, with a request to replace his missing upper right canine and first premolar with a fixed restoration.
He reported having an accident 1 year previously: An angle grinder disc had snapped and cut into his face.
The patient had sustained a full thickness laceration through the right upper and lower lips. He also sustained a dentoalveolar fracture, with traumatic luxation of the upper right canine and first premolar. The loss of teeth negatively influenced his phonetics and masticatory function, as well as his self-esteem.
A comprehensive medical and dental history was taken. This was followed by extraoral and intraoral examination.
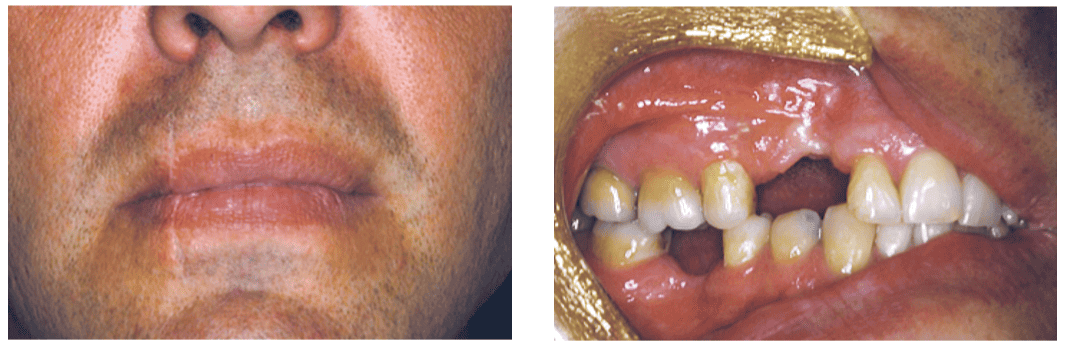
Extraoral examination revealed a vertically orientated scar, about 4 cm in length, extending across both the upper and lower lips from the inferior aspect of the right nasal ala (Figure 1). Intraoral examination revealed a healthy periodontium and no dental disease. A large volume hard and soft tissue defect was noted in the first quadrant between the UR5 and UR2 (Figure 2).
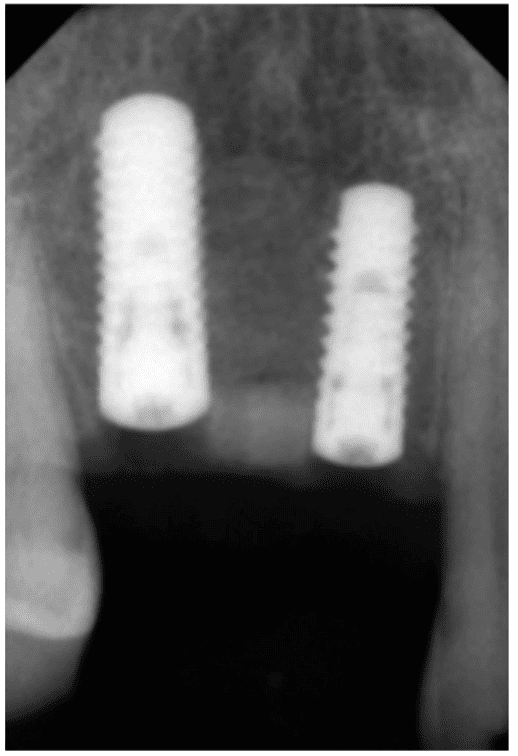
A cone beam computed tomography (CBCT) scan was done as an adjunctive diagnostic aid. This scan revealed the presence of a mini-plate and screws in the region of the healed fracture and graphically demonstrated the hard tissue defect that existed in both the vertical and horizontal dimensions (Figure 3). Reduced bone height along the proximal surfaces of teeth UR5 and UR2 was noted.

Treatment planning
The patient was assessed by a periodontist and a prosthodontist. Teeth UR5 and UR2 were not considered suitable abutment teeth for a four-unit bridge. The hard tissue defect precluded the ideal three-dimensional placement of dental implants to replace teeth UR4 and UR3.
Augmentation of the site with autogenous bone blocks, followed by a healing period of 4 to 6 months, and then placement of dental implants was considered to be the treatment of choice.
The treatment protocol was based on a consensus statement of the third ITI conference (Chen, et al., 2009), which states that “Augmentation utilizing autogenous blocks with or without membranes results in higher gains in ridge width and lower complication rates than use of particulate materials with or without membranes.” The surgical SAC assessment was graded as complex and the restorative SAC assessment as advanced (Dawson, et al., 2009).
Bone augmentation surgery
Under local anesthesia and sedation, bone blocks were harvested from the right external oblique ridge and ascending ramus of the mandible. A piezoelectric knife was used to harvest the bone (Figure 4).
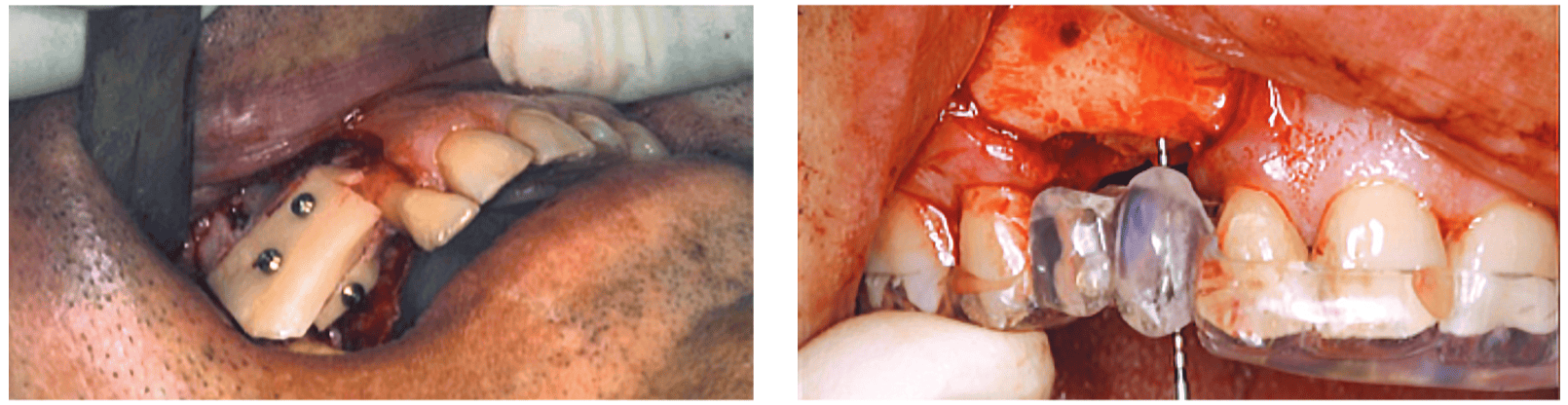
One bone block was fixed to the lateral aspect and a second bone block to the superior aspect of the deficient residual ridge using bone screws (Figure 5). Guided bone regeneration was performed by covering the bone blocks with anorganic bovine bone mineral and a collagen membrane as described by von Arx and Buser (2006). Tension-free primary closure was obtained with 5-0 nylon sutures. Postoperative medication included a chlorhexidine mouthwash, antibiotics, anti-inflammatories, and analgesics.
Dental implant surgery
Following a healing period of 4 months, the bone screws were removed and Straumann® bone level implants were inserted in teeth UR4 and UR3 positions. A prefabricated surgical stent (Figure 6) was used as a guide for the ideal three-dimensional placement of the implant fixtures (Figure 7). Closure screws were placed and primary closure obtained, and a further 2 months of healing was allowed.
Implant exposure
The implants were exposed 2 months later utilizing the roll-back technique (Figure 8).
Osseointegration of the implants was verified with a RFA monitoring instrument, yielding an adequate Implant Stability Quotient (ISQ) reading at implant level and healing abutments placed.

Prosthodontic phase
Following a further healing period of 2 weeks, implant-level impressions were taken and temporary acrylic restorations manufactured. A period of 2 months was allowed for soft tissue training to optimize the emergence profiles of the crowns. Screw-retained porcelain-fused-to-metal crowns were subsequently manufactured (Figure 9).
Discussion
Traumatic injuries as a result of work-related injuries occur frequently, with the most common sites injured by angle grinders being the head and face (Rodriguez and Guerrero, 2010; Black, et al., 2000; Carter, et al., 2008; Senthilkumaran, et al., 2010; Telmon, et al., 2001).
Injury occurs when a disc shatters while rotating during use. Human error by unskilled or untrained workers and mechanical failure have been cited as being some of the most common causes (Rodriguez and Guerrero, 2010; Carter, et al., 2008). Dental trauma constitutes a significant health issue among adults with 15.5% reporting a history of injury to the mouth or teeth (Locker, 2007).
Various treatment modalities have been used to replace lost anterior teeth, including removable partial dentures and bonded or cementable fixed bridges. With increasing patient demands, the use of removable partial dentures is rarely the option of choice as a definitive solution. Clinical follow-ups of teeth supplied with single crowns or included as abutments in bridge works have indeed demonstrated that pulp tissue necrosis is not a rare complication and may affect 10%-20% of the observed teeth over a 10- to 15-year period (Bergenholtz and Nyman, 1984).
Survival rate of implants placed in horizontally augmented bone is high (Chen, et al., 2009). Nevins, et al. (1998), in a systematic review, found that implants placed in regenerated bone had similar survival rates to implants placed in native bone.
In the repair of alveolar bone defects, intraoral donor sites offer a number of advantages. The proximity of the recipient and donor sites makes it ideal for outpatient implant surgery because less operative and anesthetic time is required. There is also no cutaneous scar, and patients report reduced morbidity and discomfort compared with extraoral locations (Schwartz-Arad and Levin, 2005; Gungormus and Yavuz, 2002).
Conclusion
The use of autogenous onlay block grafting from intraoral sites is a predictable treatment modality for reconstruction of large volume alveolar bone defects. Esthetics, function, and phonetics can be restored following trauma to the anterior maxilla by guided bone regeneration and dental implant placement.
Acknowledgments
The authors would like to thank Dr. Ashana Harrypersad, Department of Prosthodontics, University of Pretoria for the outstanding prosthodontic work.
While dental injuries from an angle grinder may be an unusual occurrence, implant dentists need to stay vigilant on technologies that can facilitate positive outcomes daily. Read Dr. Michael Hartman’s article on dynamic navigation and its benefits here.
References
- Back DL, Espag M, Hilton A, Peckham T. Angle grinder injuries. Injury. 2000;31(6):475-476.
- Bastone EB, Freer TJ, McNamara JR. Epidemiology of dental trauma: a review of the literature. Aust Dent J. 2000;45(1):2-9.
- Bergenholtz G, Nyman S. Endodontic complications following periodontal and prosthetic treatment of patients with advanced periodontal disease. J Periodontol. 1984;55(2):63-68.
- Carter LM, Wales CJ, Varley I, Telfer MR. Penetrating facial injury from angle grinder use: management and prevention. Head Face Med. 2008;4:1.
- Chen ST, Beagle J, Jensen SS, Chiapasco M, Darby I. Consensus statements and recommended clinical procedures regarding surgical techniques. Int J Oral Maxillofac Implants. 2009;24(suppl):272-278.
- Dawson A, Chen S, Buser D, et al. In: Dawson A, Chen S, eds. The SAC Classification in Implant Dentistry. Berlin, Germany: Quintessence Publishing Co; 2009.
- Glendor U. Aetiology and risk factors related to traumatic dental injuries — a review of the literature. Dent Traumatol. 2009;25(1):19-31.
- Güngörmüş M, Yavuz MS. The ascending ramus of the mandible as a donor site in maxillofacial bone grafting. J Oral Maxillofac Surg. 2002;60(11):1316-1318.
- Koyuturk AE, Kusgoz A. Multiple dentoalveolar traumatic injury: a case report (3 years follow up). Dent Traumatol. 2008;24(4):e16-e19.
- Locker D. Self-reported dental and oral injuries in a population of adults aged 18-50 years. Dent Traumatol. 2007;23(5):291-296.
- Nevins M, Mellonig JT, Clem DS 3rd, Reiser GM, Buser DA. Implants in regenerated bone: long-term survival. J Periodontics Restorative Dent. 1998;18(1):34-45.
- Rodriguez JH, Guerrero JS. Maxillofacial penetrating injury by a grinding disc: a case report. J Calif Dent Assoc. 2010;38(11):811-813.
- Schwartz-Arad D, Levin L. Intraoral autogenous block onlay bone grafting for extensive reconstruction of atrophic maxillary alveolar ridges. J Periodontol. 2005;76(4):636-641.
- Senthilkumaran S, Balamurgan N, Arthanari K, Thirumalaikolundusubramanian P. Penetrating head injury from angle grinder: a cautionary tale. J Neurosci Rural Pract. 2010;1(1):26-29.
- Telmon N, Allery JP, Scolan V, Rouge D. Fatal cranial injuries caused by an electric angle grinder. J Forensic Sci. 2001;46(2):389-391.
- von Arx T, Buser D. Horizontal ridge augmentation using autogenous block grafts and the guided bone regeneration technique with collagen membranes: a clinical study with 42 patients. Clin Oral Implants Res. 2006;17(4):359-366.
Stay Relevant With Implant Practice US
Join our email list for CE courses and webinars, articles and mores
