Dr. Moss Osman demonstrates the treatment of a patient with worn and damaged teeth
Educational aims and objectives
This article aims to discuss the rationale for the All-on-4 treatment concept of providing
implant-supported dentures and demonstrate a successful case study.
Expected outcomes
Implant Practice US subscribers can answer the CE questions to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
• Recognize the benefits of All-on-4 therapy.
• Realize the indications and limitations of this application.
Many edentulous patients suffer from having to wear a conventional complete denture and would much prefer to have a fixed implant-supported bridge instead (Strassburger, Kerschbaum, and Heydecke, 2006). One possible form of therapy is the All-on-4® treatment concept designed by Professor Paulo Maló, which enables restoration of edentulous jaws without augmentation procedures (Maló, et al., 2014).
This involves placing two straight implants in the anterior region and two angulated implants in the posterior region — the distal implants are placed diagonally at an angle of 30° to 45°. Ultimately, this treatment modality requires fewer sites, so each implant can be placed in a more optimum position. This biomechanical approach has advantages over conventional rehabilitation of the edentulous arch where eight implants are placed with external sinus augmentation.
Advantages of the All-on-4 treatment concept follow:
- Minimal or no bone augmentation is required.
- No sinus augmentation is required.
- Only four implants are needed in the mandible or four to six implants in the maxilla.
- It can be immediately restored with a provisional bridge.
- Existing bone can be optimally used.
- Vital anatomical structures can be avoided.
Studies have shown excellent outcomes for both tilted and axial implants; indeed, this protocol facilitates use of longer implants, improves bone anchorage, and avoids bone grafting procedures (Malò, at al., 2014).
This protocol facilitates use of longer implants, improves bone anchorage, and avoids bone grafting procedures.
A retrospective clinical study showed important results using two posterior tilted implants and two anterior non-tilted ones with the All-on-4 treatment concept.
Many authors have reported reduced surgical invasion (compared to alternatives such as sinus grafting surgery), shorter treatment time, lower cost, natural esthetic profiles, functional bite, and easier repairability.
Baseline situation
A patient presented at the practice looking to explore the options available for replacing his broken-down dentition. The main concerns were the shape, color, and general position of his teeth. The teeth were uncomfortable, and because he could not eat properly, he had a limited choice of foods. In addition, he lacked confidence socially and felt he had the teeth of an “older man.” Although the medical history was clear, the tooth fracture and loss were related to general lack of attention. After verbal consent was obtained, an intraoral examination was performed as well as comprehensive periodontal and dental charting, including full-mouth periapical imaging and a panoramic radiograph.
In addition to addressing the needs and expectations of the patient, all alternative treatment options available were discussed, which included both fixed and removable options:
- Full dentures
- Overdenture
- Eight implants with extensive bone and sinus grafting, implant placements with fixed porcelain bridges
- All-on-4 treatment concept with immediate fixed provisional bridge placement.
A dilemma often presents itself in these cases when extracting teeth that are potentially salvageable. It is very important for the patient to have full understanding of the treatment and consent.
After exploring the advantages and disadvantages of all options, the patient decided upon an implant-based solution for both arches.The patient wished to avoid advanced grafting techniques and didn’t want to be left without teeth at any stage of the treatment, so the All-on-4 treatment concept of implant therapy was chosen, based on the evidence of Malò and colleagues, which required sacrifice of remaining teeth and alveolar bone reduction beyond the smile line (2014).
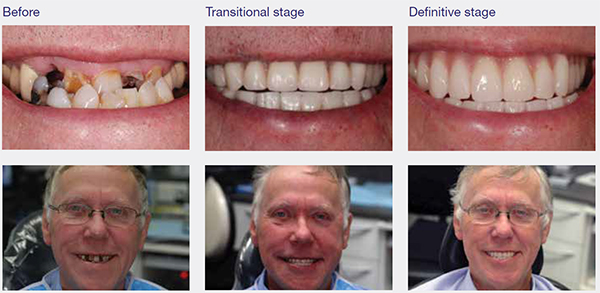




Upper and lower full acrylic dentures were then constructed, which would allow for in-surgery conversion to a fixed provisional bridge or provisional dentures, should implant placement torques be unsuitable following the loss of remaining teeth beyond the smile line.
Diagnosis, planning, and pre-treatment
The three-dimensional image from CBCT was analyzed, revealing sufficient bone volume to place five implants in the upper arch and four implants in the lower arch.
Provisional bridge/denture construction
This stage was completed by a clinical technician. Paramount consideration was given to occlusion and esthetics during construction of the provisional bridge. Primary impressions were taken with alginate, including a facebow record for a transfer to the horizontal plane. The wax rim was adjusted to ensure correct incisor length, lip support, and buccal contour in the posterior region to prescribe the buccal corridor width.
After primary impressions with stock trays, special trays and bite blocks were created to register the occlusion and assess the increase in vertical dimension. The working models were casted and articulated using the facebow. Then the teeth were removed from the working model and the amount of alveolar bone reduction anticipated. Thereafter, acrylic teeth were positioned at the new vertical dimension for the fixed prosthesis.
Construction of the provisional bridge was performed by the clinical technician — this is very helpful as it removes a large component of guesswork from the esthetics. When all parameters of esthetics and occlusion were precise, the denture/bridge was processed ready for the implant stage.
Surgical procedure
After extraction of the teeth and roots, the sockets were debrided and vertically reduced to obtain a wide bony bed around the implant shoulder. The five implants (NobelActive™, Nobel Biocare®) were inserted in the planned positions immediately after reduction of the alveolar ridge. Due to its specific design, the NobelActive implant “compresses” the bone during insertion, achieving a high level of primary stability even in compromised bone situations. The existing jawbone was maximally utilized for anchoring the implants, which were inserted as planned.
The implants placed, 4.3 mm x 13 mm, can be seen on the panoral radiograph with corresponding multi-unit abutments angulated by 0° to 35°. The required primary stability was achieved for all five implants in the upper arch and four implants in the lower arch. All had insertion torque of above 35Ncm, taken to be acceptable for immediate loading, and so immediate loading was possible.
Immediate restoration
The dental technician had prepared the provisional resin dentures for both the upper and lower arch prior to surgery. After the implants and the multibase abutments were placed, the temporary acrylic dentures were placed to check occlusion, esthetics, and smile line. Implant positions were marked on the dentures, and access holes were created. Temporary cylinders were fitted, and a rubber dam was placed to prevent the cold-cure acrylic from attaching to the suture. A quick-setting acrylic material was used to secure the cylinders within the provisional bridge. The provisional was then precisely adapted to the implant positions, and a 12-unit was immediately loaded on the provisional resin bridge for the upper and lower arch.


During the healing phase, it was important for the patient not to exert too much force during function. Acrylic provisional bridges were created without metal substructures, meaning excessive pressure could cause the provisional to break. To help prevent this and aid success of the implants, night guards are usually provided. Only soft food was advised during the healing phase of 3 months, and the dangers of load pressure were explained to the patient. The patient was reviewed 2 days later with no pain, swelling, or side effects and was very pleased with the results.
A follow-up visit was scheduled 2 weeks after surgery; the provisional bridge was checked and cleaned, and unresorbed Vicryl® (Ethicon, Inc.) sutures were removed. Also, parafunction activity was checked while provisional restoration was worn.
Final restoration
After 3 months of healing, construction of the final bridge was underway. The dental technician planned the final bridge on the basis of the provisional restoration. In general, we attempt to raise patients’ awareness of the appearance in the early provisional stages, when discussing the possible outcome. The titanium framework was precision-milled via NobelProcera® and injectable acrylic. About 4 months after surgery, the definitive bridge was placed. At the same time, the second acrylic bridge without milled bar was created as a provisional for emergency use.
Definitive work
Using the impressions taken on the placement day, working models were created, and a silicone index of the provisional teeth was used to fabricate bite blocks. In addition, we made a special tray using double thickness light-cured tray material to optimize the rigidity. By using the index of the implants into which we had placed the impression copings, we were able to put the access holes in exactly the correct position.
Impressions and initial bite
The upper provisional was removed, and the multi-abutments were checked. Impression copings were placed and splinted with stainless steel metal and composites to prevent the impression post being distorted. An impression was then taken. The occlusal registration was performed and incisal length, vertical dimension, midline, and lip profile were assessed. In the impressions, abutment analogues were placed, and a plaster base was poured to create final working models.
Wax trial
A wax try-in was constructed using a silicone index taken of the teeth. This stage was completed in the presence of the technician who also examined all the areas. Any alteration either requested by the patient or me was rectified by the technician. With the patient’s approval, we proceeded to the metal work. The framework was milled by CAD/CAM. The accuracy of fit was checked at all abutments, and the interarch relations were confirmed and recorded.
At this stage, the shade prescription was determined — restoring both the upper and lower arch afforded freedom to choose the tooth color, and the patient decided on A1. Gingival shade tabs (Ivoclar Vivadent) were used to help communicate the pink acrylic required.
Trial
The occlusion was adjusted in order to obtain a mutually protected occlusal scheme, and then the esthetics were concentrated on. Key esthetic parameters such as incisal tip placement, midline, lower lip reflection, and buccal corridors were all fine.
Fit
With both a lighter and wider smile, the display of tooth and gingival contour were harmonious. All esthetics and occlusal parameters were checked, and finally, the upper and lower bridges were torqued according to the manufacturer’s instruction. The patient is under review every 3 months at present to make sure oral hygiene is maintained.
Conclusion
In traditional dental implant therapy, the time between implant placement and delivery of the definitive prosthesis can be long and uncomfortable for a patient wearing a conventional removable denture. The All-on-4 treatment concept uses tilted implants to immediately restore maxillary and mandibular implants with provisional restorations, thus shortening the patient’s return to function, reducing surgical invasion (sinus grafting surgery), shortening treatment time, lowering cost, and enhancing natural esthetic profiles and functional bite.
The high cumulative implant and prostheses survival rates indicate that the All-on-4 treatment concept with immediate-function, combined with Nobel Biocare implant systems, is a viable treatment modality for completely edentulous mandibles.The case that suggests immediate loading associated with tilted implants prosthesis can be considered a viable treatment modality for the edentulous upper and lower arch.
References
- Strassburger C, Kerschbaum T, Heydecke G. Influence of implant and conventional prostheses on satisfaction and quality of life: A literature review. Part 2: Qualitative analysis and evaluation of the studies. Int J Prosthodont. 2006;19(4):339-348.
- Maló P, de Araújo Nobre M, Lopes A, Ferro A, Gravito I. All-on-4® Treatment Concept for the Rehabilitation of the Completely Edentulous Mandible: A 7-Year Clinical and 5-Year Radiographic Retrospective Case Series with Risk Assessment for Implant Failure and Marginal Bone Level. Clin Implant Dent Relat Res. 2015;Oct;17 Suppl2:e531-541.

