Educational aims and objectives
The aim of this article is to discuss the implementation and uses of dynamic navigation implant surgery in a modern-day dental practice.
Expected outcomes
Implant Practice US subscribers can answer the CE questions by taking the quiz to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
- Recognize differences between the two methods of surgical guidance — static guides and dynamic navigation.
- Identify the characteristics of dynamic navigation and how it works.
- Identify the other technologies needed to utilize dynamic navigation.
- Realize the characteristics of an ideal guide for dental implant placement.
Dr. Michael Hartman discusses a technology that can have a positive effect on implant treatment outcomes
Abstract
The dental implant surgeon is becoming more and more restoratively focused. Digital technology allows virtual treatment plans to be created and replicated with great accuracy during dental implant surgery with the use of dynamic navigation. When implemented with an efficient workflow, the use of dynamic navigation leads to enhanced profitability and predictably of treatment outcomes in a modern dental implant surgery practice.
 Introduction
Introduction
Digital technology is drastically changing the landscape for dental implant surgeons to develop a restoratively driven mindset. Through the use of dental implant treatment planning software, data sets from a CBCT and an intraoral scanner can be merged to create a precise virtual treatment plan. This virtual treatment plan can be carried out in an accurate manner using surgical guidance. The two methods of surgical guidance available for dental implant surgery are static guides and dynamic navigation. Both forms have similar accuracies that are superior to freehand dental implant placement.1 When comparing angular deviation between freehand and dynamic guided surgery, it was noted the average deviation was 7° buccal angle deviations for the former compared to 3° buccal angle deviations to the latter2 (Figure 1). Deviations from the planned surgery can result in less than optimal results, and damage may occur to adjacent vital structures such as roots, nerves, or sinus cavities.3 Restoring a dental implant not placed with the restorative component in mind may lead to poor esthetic results and higher laboratory costs due to the need for custom prosthetic components. It can be overwhelming to an implant practitioner to research, implement, and develop a workflow that will be not only time efficient but cost-effective while also improving patient outcomes. This article intends to outline how the role of dynamic surgical navigation enhances the predictability, profitability, and efficiency within a modern dental implant surgery practice.
What is dynamic navigation?
Dynamic navigation is a system that allows the surgeon to visualize in real time implant site development on the virtual plan as the implant drills are in function.4 Figure 2 shows the information displayed during implant placement using the X-Guide (X-Nav Technologies, Inc., Lansdale, Pennsylvania) dynamic navigation system, which is the system that I use. Multiple views are displayed simultaneously showing depth, deviations in angulation, proximity to adjacent structures, as well as handpiece orientation. Other important information such as proposed implant diameter and length is also displayed. (The X-Point Target that allows the clinician to view the position angle and depth all on a single target instead of having to look at multiple spots on the screen is patented to this brand.)
How does X-Guide work?
Optical technologies are used in a dynamic dental implant placement system to track the patient and handpiece and display the information onto a monitor.5,6,7 The X-Guide (Figures 3 and 4) uses a passive optical system that requires tracking arrays from the patient and the handpiece to be in view of its stereo cameras so the information can be relayed to the monitor.8-16 The patient array is attached to the patient via an X-Clip (Figure 5). The X-Clip is molded onto the patient’s dentition and worn during the cone beam CT scan. Once the CBCT is acquired, the X-Clip can be removed and stored for surgery to be done at a later date. The handpiece array is compatible with multiple surgical handpieces offering flexibility to the implant surgeon. Immediately prior to surgery, the patient array is attached to the X-Clip, and the assistant proceeds with the calibration of the patient and handpiece arrays. An experienced dental assistant familiar with the system can perform the calibration in under 4 minutes. During surgery, the surgeon recalibrates the handpiece after every drill change and watches the monitor during site preparation and dental implant placement. The drill recalibration takes less than 10 seconds.
Workflow
The workflow for a dynamic navigation procedure can be broken down into three parts:
- Patient implant diagnostic appointment
- Virtual treatment planning
- Dental implant surgery
Patient implant diagnostic appointment
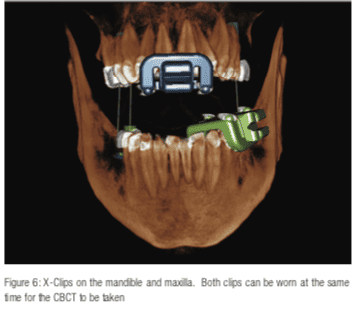
The patient implant diagnostic appointment is scheduled for 30 minutes and is usually done 2 weeks prior to surgery. During this appointment, a dental assistant molds the X-Clip onto the patient’s dentition and acquires the CBCT. Once the CBCT is verified to be free of motion distortion, the X-Clip is removed, labeled, and stored for the upcoming surgery. The X-Clip must be placed on the arch that the implant surgery will be performed. If implants are planned for both arches, both maxillary and mandibular clips may be placed at the same time for the CBCT (Figure 6). The X-Clip is placed on the opposite side of the arch from the planned surgery site. When placing anterior implants, it is preferable to place the X-Clip on the surgeon’s contralateral side. In order to ensure a firm attachment free of movement, the X-Clip itself requires three consecutive teeth to be molded onto. For instance, in a complete dentition, a right-handed surgeon would ideally have the X-Clip placed onto teeth Nos. 18,19, and 20 when placing implants in site Nos. 22-30. A similar set up would be used for the maxillary arch. When the X-Clip is placed on the surgeon’s side, it is preferable to keep it as posterior as possible to avoid interference with the implant preparation site.
 Although not required, intraoral scans may also be taken and imported in the treatment planning software. In cases where the patient does not have extensive restorative work, the scan is generally not needed. Scans would be recommended in cases with extensive restorative work (artifact on the CBCT may make ensuring the system is properly calibrated difficult.) The software allows the scans to be imported in occlusion, which may be beneficial in cases where multiple adjacent missing teeth are to be replaced. It would be ideal to acquire maxillary and mandibular scans of the surrounding planned implant areas during the patient work up appointment. A shade can also be recorded at this appointment if an immediate provisional restoration is planned.
Although not required, intraoral scans may also be taken and imported in the treatment planning software. In cases where the patient does not have extensive restorative work, the scan is generally not needed. Scans would be recommended in cases with extensive restorative work (artifact on the CBCT may make ensuring the system is properly calibrated difficult.) The software allows the scans to be imported in occlusion, which may be beneficial in cases where multiple adjacent missing teeth are to be replaced. It would be ideal to acquire maxillary and mandibular scans of the surrounding planned implant areas during the patient work up appointment. A shade can also be recorded at this appointment if an immediate provisional restoration is planned.
Virtual treatment planning
The Digital Imaging for Communication in Medicine (DICOM) data set is uploaded into the X-Guide treatment planning software. As previously mentioned, intraoral scans may be uploaded and aligned to the DICOM. If a lower posterior implant is to be planned, the inferior alveolar nerve may be mapped. The software allows for a virtual wax-up of the proposed restoration and gives the user the ability to freely move it into position and change its dimensions. Once the virtual wax-up is complete, implant planning can commence. The dental implants are planned in a generic fashion, allowing their height and width to be adjusted. In this manner, any size dental implant from any manufacturer may be planned easily.
Dental implant surgery
Once the X-Guide system is calibrated and the X-Clip is properly placed on the patient’s dentition, implant surgery can then proceed in standard fashion.
Case illustration

The patient was referred by her general dentist for evaluation of a dental implant in site No. 5. The patient had a current fixed partial denture from teeth Nos. 2, 3, 4, and 5 with a metal wing on the lingual surface of tooth No. 6. The metal wing was no longer fixated onto No. 6 (Figure 7). Evaluation revealed the bridge was still in good condition on Nos. 2, 3, and 4. After collaboration between the implant surgeon and general dentist, a treatment plan was created and presented to the patient. The treatment plan involved sectioning the bridge on the mesial of No. 4 and placing a dental implant in No 5.
After the patient’s implant diagnostic appointment, a virtual treatment plan was created (Figure 8). The plan called for the dental implant to be placed in an ideal restorative position, with the planned restoration being screw retained.
The dental implant surgery was un-eventful, and a follow-up radiograph was obtained showing the dental implant in good position (Figure 9).
Once the dental implant was osseointegrated and deemed ready to restore, a traditional impression was taken by the general dentist and sent to the dental laboratory for fabrication of a fixed screw-retained restoration. Figure 10 shows an occlusal view of the healing abutment in place with surrounding healthy gingival mucosa. Figure 11 shows the restoration and screw access hole in the middle of the occlusal surface of the crown. A screw-retained restoration was chosen due to its easy placement and retrievability if needed at a later date.
Discussion
In their article, Faurox, et al., describe the characteristics of an ideal guide for dental implant placement:
- Precision: absence of defective manufacturing, perfect fit in the mouth, high stability during operation, and optimal drill guide for a perfect reproducibility.
- The guide should be able to be stored, transported, and sterilized without distortion or degradation.
- The guide should not interfere with visual inspection or drill irrigation.
- The guide should not lead to a high-cost increase for the surgery.17
With proper case selection, a high precision of a dynamic navigation can be achieved in almost every case. From the author’s experience, in 650 cases using dynamic navigation, only two had surgeries to be changed to a freehand placement due to poorly fitting X-Clips. Satisfactory calibration was not able to be achieved due to the X-clip positions. This correlates to a 99.7% calibration success rate. In one case, the patient had a crown placed on one of the teeth that was part of the X-Clip causing the poor fit. Before the decision has been made to perform a dental implant surgery using dynamic navigation, the implant surgeon must assess where the X-Clip may be potentially placed. Teeth that exhibit mobility, loose crowns, or short root structures on radiographs should be avoided. A static guide should be considered in these scenarios.
Guides should be stored and sterilized according to the manufacturer’s recommendations. X-Clips are stored at room temperature and placed in a chlorhexidine solution prior to use. Distortion or degradation of the product has not been encountered.
A significant advantage of dynamic surgery compared to static guides is visualization of the operative field during the entire procedure. The dental assistant watches the surgical site as the implant surgeon is focused on the monitor. Unlike a static guide case, the virtual treatment plan can be modified at any time during the procedure. With a static guide, if the plan required modification, the guide would have to be aborted and either canceled or proceed in a freehand manner. Drill irrigation is not impeded with a dynamic guide system where as static guides have been shown to have increased heat production of the surrounding bone.18
Consideration should always be given to the return on investment when purchasing new technology. For example, CBCTs have a high initial cost but negligible recurring costs. It is easy for an office to estimate how many CBCTs will need to be taken before the initial cost has been recouped. This is done by dividing the cost of the machine by the amount charged per CBCT. While a dynamic navigation system may have a higher upfront cost, recurring costs are typically lower than static guides. By charging a nominal implant workup fee to the patient, the cost of the dynamic navigation unit can be recouped in approximately 280 implant cases.
Conclusion
Due to advances in digital technology combined with decreasing costs of associated hardware and software, the future is within reach for the dental implant surgeon to plan and place all dental implants using surgical guidance. The case illustrated above shows that an excellent result can be obtained through the use of creating a precise virtual treatment plan and reproducing that by utilizing dynamic navigation. This is done with a straightforward work flow and is accomplished mainly by auxiliary staff in a time-efficient manner.
Acknowledgment
The author would like to acknowledge the restorative work completed by Zachary S. Sisler DDS, Shippensburg, Pennsylvania.
Drs. Emery and Progebin have used dynamic navigation technology to prevent implant complications in their practice as well. Read about their experience.
Author Info
 Michael Hartman, DMD, MD, is an oral and maxillofacial surgeon located in Mechanicsburg, Pennsylvania. Dr. Hartman graduated from Elizabethtown College with a BS in Biology. He continued his education, earning his DMD at Temple University School of Dentistry. Dr. Hartman then completed a 6-year dual degree oral and maxillofacial surgery residency at the University of Maryland Medical Center (UMMC), earning his MD and completing his residency. Dr. Hartman has a keen interest in evolving digital technology and how it can be applied in everyday dental implant practice.
Michael Hartman, DMD, MD, is an oral and maxillofacial surgeon located in Mechanicsburg, Pennsylvania. Dr. Hartman graduated from Elizabethtown College with a BS in Biology. He continued his education, earning his DMD at Temple University School of Dentistry. Dr. Hartman then completed a 6-year dual degree oral and maxillofacial surgery residency at the University of Maryland Medical Center (UMMC), earning his MD and completing his residency. Dr. Hartman has a keen interest in evolving digital technology and how it can be applied in everyday dental implant practice.
Disclosure: The author has no financial disclosures.
References
- Block MS, Emery RW, Lank K, Ryan J. Implant Placement Accuracy Using Dynamic Navigation. Int J Oral Maxillofac Implants. 2017;32(1):92-99.
- Block MS, Emery RW, Cullum DR, Sheikh A. Implant Placement is More Accurate Using Dynamic Navigation. J Oral Maxillofac Surg. 2017;75(7):1377-1386.
- Zhou W, Liu Z, Song L, Kuo CL, Shafer DM. Clinical Factors Affecting the Accuracy of Guided Implant Surgery – A Systematic Review and Meta-Analysis. J Evid Based Dent Pract. 2018;18(1):28-40.
- Luebbers HT, Messmer P, Obwegeser JA, et al. Comparison of different registration methods for surgical navigation in cranio-maxillofacial surgery. J Craniomaxillofac Surg. 2008;36(2):109-116.
- Block MS, Emery RW. Static or Dynamic Navigation for Implant Placement – Choosing the Method of Guidance. J Oral Maxillofac Surg. 2016;74(2):267-277.
- Nijmeh AD, Goodger NM, Hawkes D, Edwards PJ, McGurk M. Image-guided navigation in oral and maxillofacial surgery. Br J Oral Maxillofac Surg. 2005;43(4):294-302.
- Bouchard C, Magill JC, Nikonovskiy V, et at. Osteomark: a surgical navigation system for oral and maxillofacial surgery. Int J Oral Maxillofac Surg. 2012;41(2):265-270.
- Strong EB, Rafii A, Holhweg-Majert B, Fuller SC, Metzger MC. Comparison of 3 optical navigation systems for computer-aided maxillofacial surgery. Arch Otolaryngol Head Neck Surg. 2008;134(10):1080-1084.
- Casap N, Wexler A, Eliashar R. Computerized navigation for surgery of the lower jaw: comparison of 2 navigation systems. J Oral Maxillofac Surg. 2008;66(7):1467-1475.
- Poeschl PW, Schmidt N, Guervara-Rojas G, et al. Comparison of cone-beam and conventional multislice computed tomography for image-guided dental implant planning. Clin Oral Investig. 2013;17(1):317-324.
- Ewers R, Schicho K, Undt G, et al. Basic research and 12 years of clinical experience in computer-assisted navigation technology: a review. Int J Oral Maxillofacial Surg. 2005;34(1):1-8.
- Wittwer G, Adeyemo WL, Schicho K, Birkfellner W, Enislidis G. Prospective randomized clinical comparison of 2 dental implant navigation systems. J Oral Maxillofacial Implant. 2007;22(5):785-790.
- Wanschitz F, Birkfellner W, Watzinger F, et al. Evaluation of accuracy of computer-aided intraoperative positioning of endosseous oral implants in the edentulous mandible. Clin Oral Implants Res. 2002;13(1):59-64.
- Leuth TC, Wenger T, Rautenberg A, Deppe H. RoboDent and the Change of Needs in Computer-Aided Dental Implantology During the Past Ten Years. Presented at the 2011 IEEE International Conference on Robotics and Automation, May 9-13, 2011. IEEE Abstracts 2011:1.
- Casap N, Laviv AW. Computerized Navigation for Immediate Loading of Dental Implants With a Prefabricated Metal Frame: A Feasibility Study. J Oral Maxillofac Surg. 2011;69(2):512-519.
- Siessegger M, Schneider BT, Mischkowski RA, et al. Use of an image-guided navigation system in dental implant surgery in anatomically complex operation sites. J Craniomaxillofac Surg. 2001;29(5):276-281.
- Fauroux MA, De Boutray MD, Malthiéry E, Torres JH. New innovative method relating guided surgery to dental implant placement. J Stomatol Oral Maxillofacial Surg. 2018;119(3):249-253.
- Dos Santos PL, Queiroz TP, Margonar R, et al. Evaluation of bone heating, drill deformation, and drill roughness after implant osteotomy: guided surgery and classic drilling procedure. Int J Oral Maxillofac Implants. 2014;(29)1:51-58.

