Dr. Shakeel Shahdad presents a clinical case illustrating replacement of a maxillary canine with a narrow diameter implant in a hypodontia patient
Implants are now considered a predictable choice to replace missing teeth; nevertheless, replacement in the esthetic zone remains a challenge.
In addition to the challenges posed by the various clinical scenarios, our patients have high expectations; they demand optimal functional and esthetic outcomes.
Educational aims and objectives
This article aims to discuss an implant method of replacing a tooth in the esthetic zone.Expected outcomes
Implant Practice US subscribers can answer the CE questions to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
- Identify a method of preoperative assessment for implant placement.
- Recognize a method to deliver a restoration that esthetically fulfills the objectives of treatment
- Recognize a method to deliver a restoration that functionally fulfills the objectives of treatment.
- See how to fulfill a specific need by using narrow diameter implant to replace a canine tooth.
An ideal implant restoration has to recreate gingival esthetics, and for a clinician, the pink esthetics remain the most challenging aspect of the treatment.
In recent years, we have become more critical in objectively assessing the outcome with newer indices. Furhauser and colleagues (2005) recommended the “pink esthetic score” (PES) as a means of objectively assessing gingival esthetics in implant restorations, especially single-tooth implants. Besides papillae, the PES combines the height, contour, color, and texture of the peri-implant soft tissues.
Achieving an ideal esthetic outcome in implant restorations requires a meticulous approach. The different stages of treatment are important, and a thorough preoperative assessment underpins the process.

To ensure an optimal outcome, the following factors are important:
- Three-dimensional surgical placement
- Esthetic hard tissue grafting
- Careful soft tissue handling during second-stage surgery
- Soft tissue sculpting with a provisional restoration
- Utilizing a technique that aids creation of an optimal definitive restoration. In this article, a clinical case illustrating replacement of a maxillary canine with a narrow diameter implant is presented in a hypodontia patient.
Clinical case

A 32-year-old male patient presented with a congenitally missing maxillary lateral incisor. Specialist orthodontic treatment had been completed elsewhere without any restorative interdisciplinary planning.
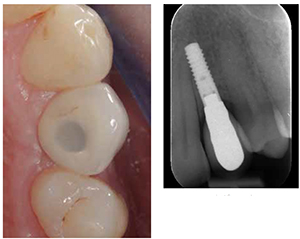
The UL3 was positioned in the UL2 space, and a pontic space was present in the UL3 area (Figure 1). A diminutive right lateral incisor was present. The overall dentition was minimally restored, and the pontic space mesiodistally was adequate for a canine width tooth (Figure 2). However, the interradicular space was limited and inadequate for replacement of this tooth with an average diameter implant, ideally suited for a canine tooth (Figure 3).
After a detailed discussion, the patient ruled out a resin-retained bridge and preferred to have the tooth replaced with a dental implant. Direct composite buildup was carried out to optimize the diminutive right lateral incisor and reshape the UL3 as the UL2.
A narrow diameter, tissue-level type, Straumann® Roxolid® hydrophilic implant (3.3 mm diameter NNC) was placed in an ideal three-dimensional position for a screw-retained single-tooth restoration. Submerged healing was allowed for 6 weeks followed by implant exposure surgery.



After a period of provisionalization to allow peri-implant soft tissue molding (Figures 4-6), impression coping was customized to facilitate the dental technician (Figures 7 and 8) to achieve an ideal emergence in the definitive restoration (Figure 9).
Conclusion
While the success of osseointegration is now an established fact, the challenge for clinicians is to deliver restorations that esthetically fulfill the objectives of treatment. This clinical case demonstrates how careful assessment and treatment planning can be predictably controlled to fulfill the treatment objectives.
A narrow diameter implant was used to replace a canine, which is now feasible to do predictably with the advent of stronger dental implant materials.
Despite the non-ideal orthodontic result, the final esthetic outcome with the dental implant and reshaping of teeth with directly bonded composite restorations yielded a great result for this patient (Figures 10 and 11).

References
- Fürhauser R, Florescu D, Benesch T, Haas R, Mailath G, Watzek G. Evaluation of soft tissue around single-tooth implant crowns: the pink aesthetic score. Clin Oral Implants Res. 2005;16(6):639-644.
- Jemt T. Regeneration of gingival papillae after single-implant treatment. Int J Periodontics Restorative Dent. 1997;17(4):326-333.
- Tarnow DP, Cho SC, Wallace SS. The effect of inter-implant distance on the height of inter-implant bone crest. J Periodontol. 2000;71(4):546-549.

