Drs. Shahram Nik and Kaveh Golab discuss the minimal postoperative discomfort when providing a patient with a fixed prosthesis immediately after implant placement
 Immediate loading of dental implants is a valuable technique that can decrease the treatment period, minimize surgical sessions, and increase patient satisfaction. In comparison with conventional techniques, immediate loading has shown same success in Cochrane reviews (Esposito, et al., 2013).
Immediate loading of dental implants is a valuable technique that can decrease the treatment period, minimize surgical sessions, and increase patient satisfaction. In comparison with conventional techniques, immediate loading has shown same success in Cochrane reviews (Esposito, et al., 2013).
One-piece implants are newly introduced implants in order to facilitate oral rehab-
ilitation and accelerate the tooth replacement procedure. With the high-tech design of these implants, it seems that using one-piece implant can satisfy both surgical and prosthetic requirements of patients.
These implants have also demonstrated long-term survival rate. They are designed with the aim of fewer complications compared with two-piece implants (Barrachina-Diez, et al., 2013; Finne, Rompen, and Toljanic, 2012; Prithviraj, et al., 2013). One-piece implants not only do not have microleakage and micromovements between abutment and fixture, but also do not have the common screw-loosening complications, according to Prithviraj and colleagues (2013).
The dentist and his/her assistant can feel relaxed in the implant clinic because these implants do not need different types of screwdrivers, stock of various abutment sizes, and collars. In addition, they are completely welcomed from meticulous patients due to precise preparation of the abutment crown with gingival margin and simplicity of provisionalization. Solid design of these implants ensure small diameter manufacturing; therefore, they can be used in the esthetic zone with adequate distance from adjacent teeth, resulting in preservation of interdental bone and gingival papillae (Sohn, 2011; Zembic, 2012). In patients with thin mucosa and possible exposure of abutment margin, the finishing line of crown preparation can be extended on solid abutment to cover the titanium surface.
One Piece Screw (OPS) implants (S&S Biomat Ltd., Manchester, United Kingdom) have threads with variable depth; they gradually increase from the coronal toward apical end (from 0.3 mm-0.03 mm). The threads on the apical area are V-shaped, which enable self-tap characteristics of the implant. These threads are transforming to Acme threads on the coronal parts of the fixture. Transmucosal parts are flared with a different gingival height size (2 mm, 4 mm), which can be selected due to the mucosal width of the site. Solid abutments have two anti-rotational elements that can be prepared same as conventional fixed prosthesis.
Material and methods
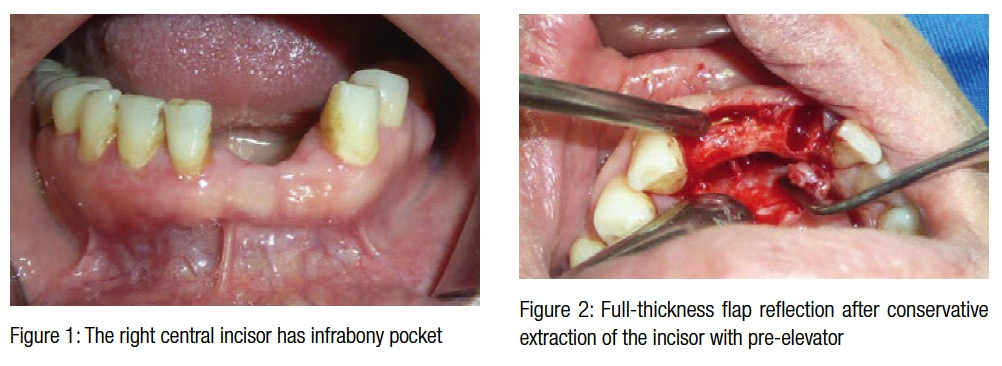
The patient in this article had severe bone resorption around mandibular anterior tooth. In addition, this tooth was mobile. The patient received antibiotics (amoxicillin and metronidazole) and an analgesic before the surgery and continued 1-week post-surgery. After a local anesthesia, the incisor was extracted using a traumatic technique with pre-elevator (S&S Biomat) to preserve remaining alveolar bone. Then the soft tissues in the sockets were carefully removed, and a full-thickness flap was reflected.
Under a copious irrigation, serial drilling of implants (Dr. Nik, S&S Biomat) was done to prepare the implant socket. The drills are specially designed to collect the bone debris in their flutes. This debris can not only indicate the quality of bone but can also be used in the case of autogenous bone grafts. After measuring of the soft tissue thickness, proper implants were selected and inserted into the socket. The inserted implants gained the 35Ncm insertion torque, which is acceptable for immediate loading of implants.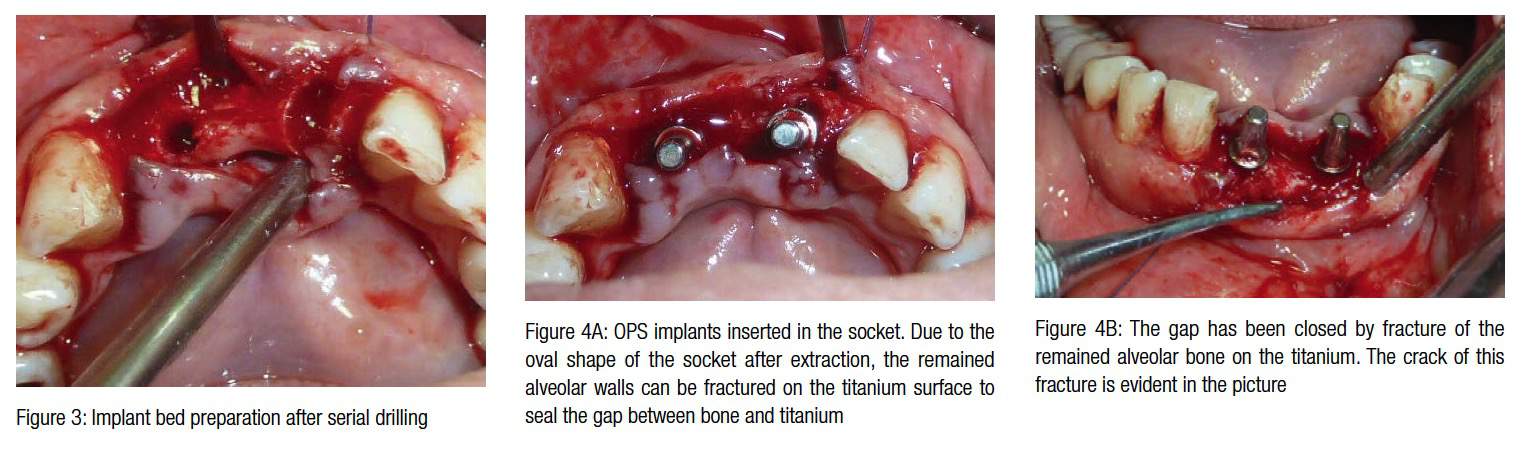
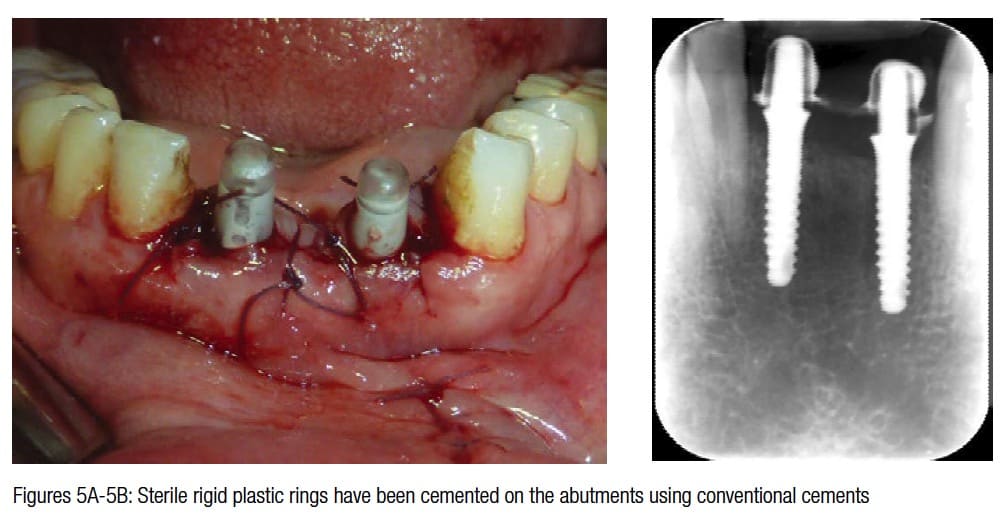
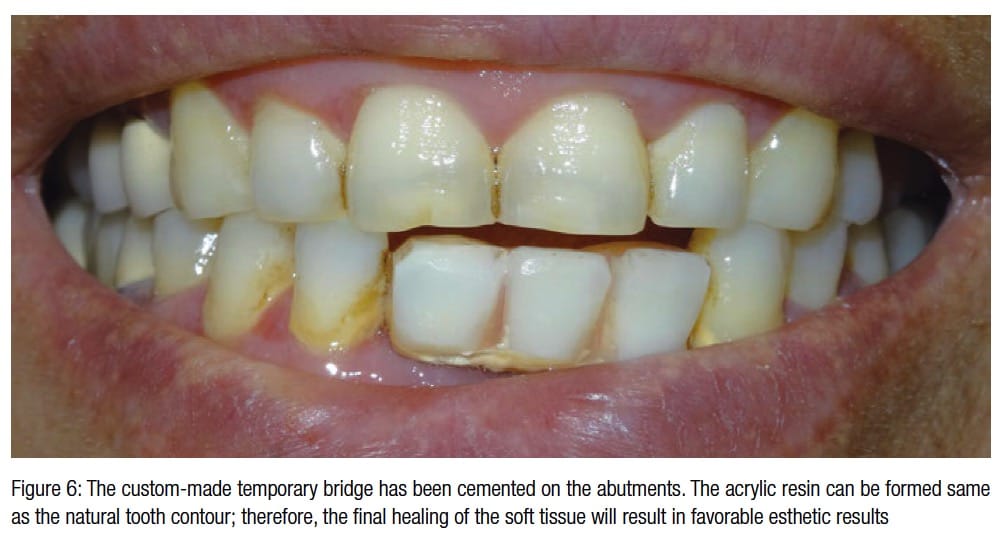
 The temporary acrylic bridge, which had been made for the patient, was relined with self-cure acrylic resin. Afterward the bridge was cemented on the abutments with zinc phosphate cement. It was trimmed in a natural way to simulate previous teeth contour, which will lead to soft tissue formation with a natural contour to be formed near crowns. Three months after insertion surgery, the implants were osseointegrated, and the abutments were prepared using high-speed carbide burs (SS White). Direct impression using additional silicones was made. A resin framework was tried in intraorally to ensure the passive fitness of the final bridge, and finally, after confirmation of the esthetic characteristics of the bridge by the patient, the bridge was cemented.
The temporary acrylic bridge, which had been made for the patient, was relined with self-cure acrylic resin. Afterward the bridge was cemented on the abutments with zinc phosphate cement. It was trimmed in a natural way to simulate previous teeth contour, which will lead to soft tissue formation with a natural contour to be formed near crowns. Three months after insertion surgery, the implants were osseointegrated, and the abutments were prepared using high-speed carbide burs (SS White). Direct impression using additional silicones was made. A resin framework was tried in intraorally to ensure the passive fitness of the final bridge, and finally, after confirmation of the esthetic characteristics of the bridge by the patient, the bridge was cemented.
Results and discussion
The implants were integrated successfully after 3 months. There was no sign of inflammation near the temporary bridge and/or implants. The patient was instructed to maintain oral hygiene. Immediate replacement of extracted teeth has the advantage of a shorter treatment period and less surgical procedures as well as resulting in better esthetic results, according to Hamouda and colleagues (2015).

It is likely after tooth extraction to encounter a remained alveolar bed with different bone level in the buccal and lingual surface of the socket. This problem can easily be solved with selection of a one-piece implant with different gingival heights. OPS implants are the only system that provides implants with variable gingival heights. The clinical point is that by considering the more apical bony wall of the remained socket as the reference point for drilling, the dentist should select a gingival height size, which can compensate for the difference between alveolar walls.
 The temporization phase of these one-piece implants helped the dentist and patient have a clear idea of the final prosthesis. Furthermore, the soft tissue maturation near the temporary bridge had the same characteristics as the natural tooth soft tissue. Implant patients have shown to prefer restoring their missing teeth rapidly (Schropp, 2004), and our patient did not experience the edentulous period. It seems that precise debridement of the sockets after conservative extraction ensured an infection-free site for successful osseointegration (Blus and colleagues, 2015).
The temporization phase of these one-piece implants helped the dentist and patient have a clear idea of the final prosthesis. Furthermore, the soft tissue maturation near the temporary bridge had the same characteristics as the natural tooth soft tissue. Implant patients have shown to prefer restoring their missing teeth rapidly (Schropp, 2004), and our patient did not experience the edentulous period. It seems that precise debridement of the sockets after conservative extraction ensured an infection-free site for successful osseointegration (Blus and colleagues, 2015).
It is necessary for the practitioner to be provided with a detailed surgery protocol to have an accurate implant bed beyond the extraction socket. The Dr. Nik Implant System has determined a simple and practical protocol with regard to the amount of bone debris accumulated in the drill flutes. It is important to examine the primary stability of the intended implant by placement of the same size drill into the socket and checking the axial stability of the drill. Implementation of this protocol guaranteed proper selection of the one-piece implant with enough primary stability. The Dr. Nik Implant System is designed for precise insertion of four types of implant with the same surgical kit. If the final drill of the implant bed preparation lacks sufficient stability in the bone, we would insert conventional two-piece screw-type implants (S&S Biomat) in the socket.
References
- Barrachina-Diez JM, Tashkandi E, Stampf S, Att W. Long-term outcome of one-piece implants. Part I: implant characteristics and loading protocols. A systematic literature review with metaanalysis. Int J Oral Maxillofac Implants. 2013;28(2):503-518.
- Blus C, Szmukler-Moncler S, Khoury P, Orrù G. Immediate implants placed in infected and noninfected sites after atraumatic tooth extraction and placement with ultrasonic bone surgery. Clin Implant Dent Relat Res. 2015;17(suppl 1):e287-297.
- Esposito M, Grusovin MG, Maghaireh H, Worthington HV. Interventions for replacing missing teeth: different times for loading dental implants. Cochrane Database Syst Rev. 2013;3:CD003878.
- Finne K, Rompen E, Toljanic J. Three-year prospective multicenter study evaluating marginal bone levels and soft tissue health around a one-piece implant system. Int J Oral Maxillofac Implants. 2012;27(2):458-466.
- Hamouda NI, Mourad SI, El-Kenawy MH, Maria OM. Immediate implant placement into fresh extraction socket in the mandibular molar sites: a preliminary study of a modified insertion technique. Clin Implant Dent Relat Res. 2015;17(suppl 1):e107-116.
- Prithviraj DR, Gupta V, Muley N, Sandhu P. One-piece implants: placement timing, surgical technique, loading protocol, and marginal bone loss. J Prosthodont. 2013;22(3):237-244.
- Schropp L, Isidor F, Kostopoulos L, Wenzel A. Patient experience of, and satisfaction with, delayed-immediate vs. delayed single-tooth implant placement. Clin Oral Implants Res. 2004;15(4):498-503.
- Sohn DS, Bae MS, Heo JU, Park JS, Yea SH, Romanos GE. Retrospective multicenter analysis of immediate provisionalization using one-piece narrow-diameter (3.0-mm) implants. Int J Oral Maxillofac Implants. 2011;26(1):163-168.
- Zembić A, Johannesen LH, Schou S, Malo P, Reichert T, Farella M, Hämmerle CH. Immediately restored one-piece single-tooth implants with reduced diameter: one-year results of a multi-center study. Clin Oral Implants Res. 2012;23(1):49-54.

