Professor Loris Prosper and Nicolas Zunica discuss a case report preventing iatrogenic damage to the inferior alveolar and lingual nerves during third mandibular molar extraction
The inferior alveolar nerve (IAN) is a sensitive nerve made of parallel nervous fibers (central/peripheric). It originates from the posterior terminal end of the posterior mandibular nerve while the lingual nerve (LN) is a branch of the mandibular division of the trigeminal nerve.
Educational aims and objectives
This clinical article aims to discuss a treatment method for prevention of iatrogenic damage
to the inferior alveolar and lingual nerves during third mandibular molar extractionExpected outcomes
Implant Practice US subscribers can answer the CE questions to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
- Identify several types of inferior alveolar and lingual nerve injuries.
- Recognize some symptoms of iatrogenic nerve injuries.
- Realize some significant risk factors for IAN damage.
- Realize some surgical factors that may result in permanent lingual nerve injury.
 The IAN and the LN are the nerves presenting more risk of unintended iatrogenic injury lesion during mandibular molar extraction. These nerve injuries were first classified in 1943 in three categories (Sunderland, 1951; Andrew and Churchill, 1991; Greenberg, 1994).
The IAN and the LN are the nerves presenting more risk of unintended iatrogenic injury lesion during mandibular molar extraction. These nerve injuries were first classified in 1943 in three categories (Sunderland, 1951; Andrew and Churchill, 1991; Greenberg, 1994).
Neuropraxia: An interruption in conduction of the impulse down the nerve fiber. The recovery in such cases takes place without Wallerian degeneration; hence, it is considered to be the mildest form of nerve injury.
Axonotmesis: Loss of the relative continuity of the axon and its covering of myelin, but preservation of the connective tissue framework of the nerve.
Neurotmesis: Loss of continuity of not only the axon, but also the encapsulating connective tissue.
The International Association for Study of Pain (IASP) distinguished the following symptoms:
- Anesthesia: total absence of sensibility
- Paresthesia: alteration of sensibility implying a sensation of tingling, tickling, prickling, pricking, or burning
- Hypoesthesia: a reduced sense of touch or sensation, or a partial loss of sensitivity to sensory stimuli
- Hyperesthesia: a condition that involves an abnormal increase in sensitivity to stimuli
- Dysesthesia: abnormal sense of touch involving sensations such as burning, wetness, itching, electric shock, and pins and needles.
The incidence of reported postoperative damage to the IAN and LN varies widely in the literature. A 2005 survey involving all oral surgeons in California and aiming to estimate the occurrence of neurologic damage to the inferior alveolar and the lingual nerve surgical shows that 94.5% of the 535 surgeons answering the survey reported damage to the inferior alveolar nerve and 56% to the lingual nerve (Robert, Bacchetti, and Pogrel, 2005).
In a study published by Gargallo-Albiol and colleagues, the incidence of temporary disturbances affecting the IAN or the LN was found to be in the range from 0.278% to 13% (2000). In another study by Zuniga, the incidence of permanent injury to the IAN and LN has been mentioned to fall in the range between 0.4% and 25% and 0.04% and 0.6%, respectively (2009).
 Risk factors
Risk factors
Two important factors can significantly increase the risk of IAN damage: anatomy and old age. By anatomy, we mean the relationship between neurovascular bundle and roots of the third mandibular tooth, identifiable through orthopantomogram (OPG). As early as 1990, Rood and Shehab identified a list of clear indications for significantly higher risks for the inferior alveolar nerve, all identifiable through OPG. See Table 1 “Indicators of risk factors of IAN damage” for more information.
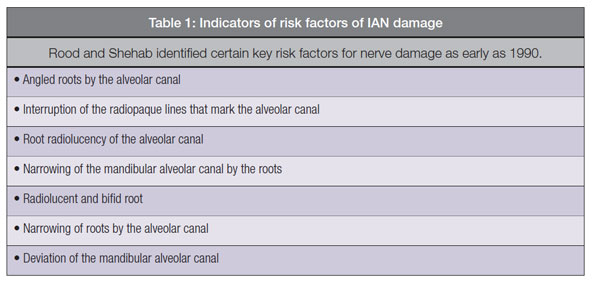 The importance of these risk indicators was recently confirmed by Blaeser and colleagues (2003), who calculated the value of some of Rood and Shehab’s indicators, such as:
The importance of these risk indicators was recently confirmed by Blaeser and colleagues (2003), who calculated the value of some of Rood and Shehab’s indicators, such as:
- Deviation of the mandibular alveolar canal
- Root radiolucency
- Interruption of the radiopaque lines that mark the alveolar canal.
In the presence of these conditions, the neurologic damage is between 1.4% and 2.7%, so at least 40% higher than the general risk probability. Sedaghafar and colleagues take the clinic-radiographic evaluation a step further, showing that the damage forecast is even more accurate if further information is taken into account such as the development of roots and their shape, deepness of the inclusion, etc. (2005; Rood and Shehab, 1990).
 A study carried out by Andrew and Wee to determine the incidence of inferior alveolar nerve paresthesia during third molar surgery in patients with an exposed inferior alveolar nerve bundle concluded that such a situation hints a high probability of intimate relationship of the nerve with the tooth and carries a 20% risk of paresthesia with a 70% chance of recovery by 1 year from surgery (2004).
A study carried out by Andrew and Wee to determine the incidence of inferior alveolar nerve paresthesia during third molar surgery in patients with an exposed inferior alveolar nerve bundle concluded that such a situation hints a high probability of intimate relationship of the nerve with the tooth and carries a 20% risk of paresthesia with a 70% chance of recovery by 1 year from surgery (2004).
 The patient’s age
The patient’s age
The patient’s age is another significant risk factor. The literature shows that post-extraction complications are more frequent after the age of 25 (Chuang, et al., 2007; Bruce, Frederickson, and Small, 1980; Chiapasco, De Cicco, and Marrone, 1993). A recent retrospective survey carried out on 4,995 extractions performed on 3,513 patients reported neurologic damage in 55 cases (1.1%). Most of the times, the damage was reversible, but 50% of patients recovered in 6 months; in some cases, it took over a year to recover full sensibility. A partial recovery of sensibility was more frequently observed in older patients (Queral-Godoy, et al., 2005).
Preoperative diagnosis
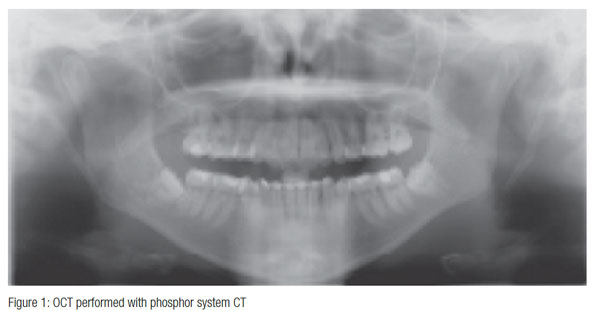
Preoperative diagnosis includes ortho-pantomogram (OPG) and three-dimensional imaging. OPT clearly shows the tooth position, eventual diseases such as caries and cysts, and risks for the mandibular alveolar nerve according to Rood and Shehab’s indicators (complete overlapping of the roots to the alveolar canal, alveolar canal that crosses the roots near to the bifurcation) but does not show the buccolingual position of roots and neurovascular bundle.
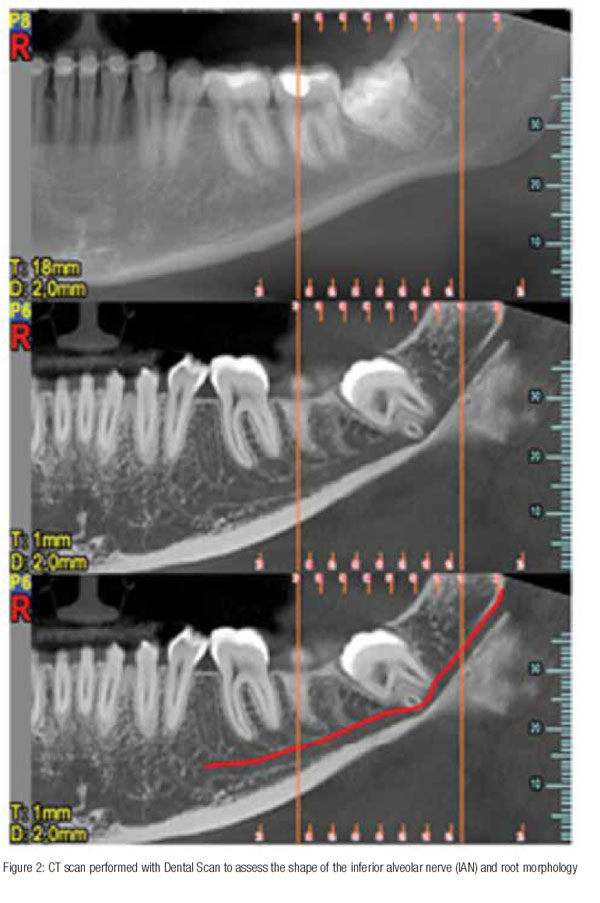
Three-dimensional imaging and particularly cone beam technology proves very useful by indicating the exact position of the alveolar canal and allows for planning of a correct bone resection and odontotomy. Three-dimensional imaging is seldom indicated for patients below 25 years of age because there are less risks of neurologic damage and because there is generally less need for extraction instruments to penetrate as deep in the root apex.
Surgical factors
While several studies come to the general conclusion that the deeper the third molar, the higher the rate of nerve damage, other authors stress the importance of surgical factors as being significant contributors to nerve injury. An investigation carried out in 2001 by Renton and colleagues concluded that the predictors for permanent lingual nerve injury, in order of importance, were perforation of the lingual plate during surgery, the skill of the surgeon, difficulty of the case (distoangular impactions), exposure of the nerve, and an increased age of the patient. The authors further stated that the surgical factors are the main contributors to lingual nerve injury during third molar extraction (2001).
Some authors even conclude that, rather than the mandibular depth of third molar, the true cause of nerve damage is the surgical maneuver required during extraction such as lingual flap retraction, osteotomy, and tooth sectioning (Carmichael and McGowan, 1992; Fielding, Rachiele, and Frazier, 1997; Waseem, et al., 2010; Mason, 1988). The technique used would, in other words, determine at least to some extent the probability of nerve injury.
Case report
Instruments and methodology
Extraction technique when removing an impacted or semi-impacted mandibular third molar is extremely important in order to prevent damage to the surrounding anatomical structures such as the lingual nerve, the inferior alveolar nerve, and the periodontium of the second molar.
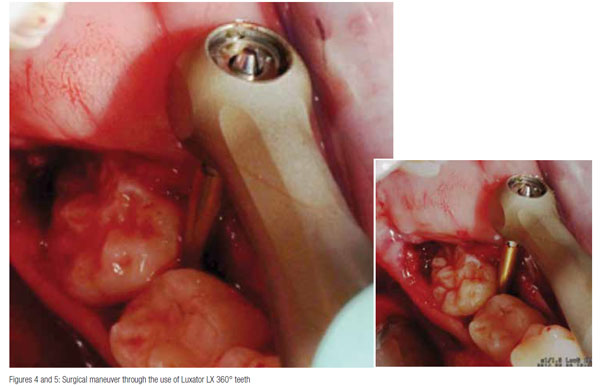
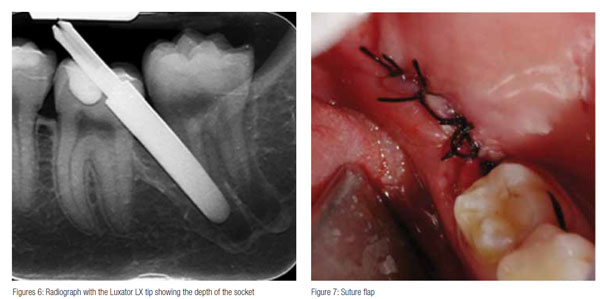
The surgical instruments used are of paramount importance. In the case that follows, an innovative instrument, the mechanical periotome Luxator LX® (Directa) was used to perform a mandibular third molar extraction. The instrument allows to cut the Sharpey fibers surrounding the tooth between cement and alveolar bone (Feneiss, et al., 1952) by luxating the periodontal ligament as seen in Figures 4 to 6.
Presentation
The patient was a 22-year-old female in good health. She visited our clinic in Monza (Italy), reporting pain coming from the LL8 and spreading through the whole lower arch. The first panoramic picture shows compression of the mandibular nerve that touches the lower roots of the LL8 — physical inclusion of the mucosa and partial bone inclusion in close correlation with the inferior alveolar nerve. Physical examination showed edematous and erythematous mucosa distal to the LL7. No sensibility alteration in the emiarch concerned. A second X-ray showed the position of the inferior alveolar nerve at the distolingual apex as confirmed by CT.
Treatment
The patient was given anesthesia and plexus nerve block with a 2% vaso-constrictor. The LL8 was exposed, and an intrasulcular incision with drainage to the LL7 was made. The distal discharge should be performed at a 45° angle to the second molar, remaining in the first portion of a full thickness, then finished at partial thickness. This incision avoids the risk of sectioning the lingual nerve and is the junction of the flap.
After skeletonizing the jaw and placing tongue protection, the Sharpey’s fibers were cut using the mechanical periotome Luxator LX following the tooth circumference and luxating the periodontal ligament as in Figures 4 and 5. The tooth is subsequently extracted using an elevator without luxating the surrounding tissues and, above all, with no damage to the mandibular nerve.
The controlled reciprocating movement of the Luxator LX helps it penetrate the space that lodges the periodontal ligament (0.15 mm-0.38 mm) and separates the fiber bundle in the least traumatic way for the tooth. The gentle vertical movement applied to the periodontium does not cause neural trauma. Using this mechanical periotome, we managed to perform the extraction with no tissue damage and, most importantly, with no damage to the mandibular nerve.
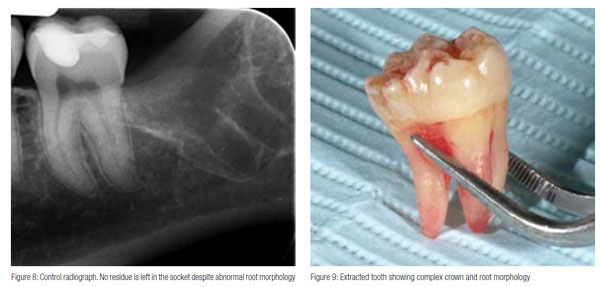
The periapical X-ray (Figure 6) shows how the Luxator LX blade — detached from the contra-angle to facilitate the X-ray — penetrates into the alveolus facilitating tooth removal. Figure 8 shows the absence of root rests. The extraction was performed without sectioning/dividing the tooth. Figure 9 shows that the tooth was extracted in one piece. No traumatic operations to search for root rests were needed.
The alveolus was cleaned, washed with cold physiologic solution, and sutured with silk thread 4/0-. The edge could be sutured enabling the patient to recover without postoperative pain. Seven days later, the suture stitches were removed. The patient reported a good postoperative recovery with slight pain during the first 3 days mitigated by common painkillers.
The patient was instructed to use a toothpaste gel (Hobagel by Hobama) that contains a mix of humectant and antibacterial substances (such as cetylpyridinium chloride, triclosan, essential oils) in technologically innovative microcapsules designed to significantly lower periodontal plaque and bleeding. Its medium-low RDA (+/-30) is less abrasive on natural tooth and restoration material (Pasini, et al., 2012).
The dental hygienist should focus on reducing plaque close to the postoperative recovery areas, detect poor home hygiene, and promptly intervene to correct them. Professional dental hygiene sessions are extremely important to remove bacteria around the tooth, preferably by air polish (EMS) with glycine powder to preserve the health of gingival tissues. Final polishing is of extreme importance to leave a smooth surface as a rough surface will be more receptive for bacteria. A silica-based polishing paste with a low RDA such as prophy paste CCS Yellow RDA 40 (Directa) is recommended (Prosper, et al., 2013).
 Conclusion
Conclusion
Mandibular third molar extractions are undoubtedly associated with neural injury risks that can cause temporary or permanent discomfort for the patient and legal actions for the dentist.
A thorough preoperative diagnosis is mandatory, and complication factors such as age and anatomy — i.e., depth of impaction and presence of overlying ramus bone — need to be taken into account.
The surgical approach used is of paramount importance to minimize tissue damage and neurosensory impairment. The mechanical Periotome Luxator LX proves to be a valid tool in surgical extractions allowing minimal trauma and significant reduction of postoperative discomfort.
References
- Andrew BGT, Wee SG. Effect of exposed inferior alveolar neurovascular bundle during surgical removal of impacted lower third molars. J Oral Maxillofac Surg. 2004; 62(5):592-600.
- Andrew K, Churchill L. Classification of nerve injuries. Essential Neurosurgery. 1991; 333-334.
- Blaeser BF, August MA, Donoff RB, Kaban LB, Dodson TB. Panoramic radiographic risk factors for inferior alveolar nerve injury after third molar extraction. J Oral Maxillofac Surg. 2003; 61(4):417-421.
- Bruce RA, Frederickson GC, Small GS. Age of patients and morbidity associated with mandibular third molar surgery. J Am Dent Assoc. 1980;101(2):240-45.
- Carmichael FA, McGowan DA. Incidence of nerve damage following third molar removal: a West of Scotland oral surgery research group study. Br J Oral Maxillofac Surg. 1992;30(2):78-82.
- Chiapasco M, De Cicco L, Marrone G. Side effect complications associated with third molar surgery. Oral Surg Oral Med Oral Pathol. 1993; 76(4):412-420.
- Chuang SK, Perrott DH, Susarla SM, Dodson TB. Age as a risk factor for third molar surgery complications. J Oral Maxillofac Surg. 2007;65(9):1685-1692.
- Fielding AF, Rachiele DP, Frazier G. Lingual nerve paresthesia following third molar surgery. a retrospective clinical study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997;84(4):345-348.
- Gargallo-Albiol J, Buenechea-Imaz R, Gay-Escoda C. Lingual nerve protection during surgical removal of lower third molars. a prospective randomized study. Int J Oral Maxillofac Surg. 2000;29(4):268-271.
- Greenberg, MS. Injury Classification System. Handbook of Neurosurgery. 3rd ed. Lakeland, FL: Greenberg Graphics Inc; 1994.
- Mason DA. Lingual nerve damage following lower third molar surgery. Int J Oral Maxillofac Surg. 1988;17(5):290-294.
- Pasini G, Zorzo C, Gola G, Polizzi E. Valutazione clinica di un gruppo di pazienti, affetti da gengivite, dopo utilizzo di un gel a base di cetil- piridinio cloruro, triclosan e olii essenziali. Quintessenza Internazionale. 2012;1:23-30.
- Prosper L, Setaro I, Polizzi E, Zunica N, Cassinelli E, Cortella CA. Materiali estetici restaurativi: analisi in vistro sull’adesione batterica e danni iatrogeni indotti dalle tecniche d’igiene professionale. Quintessenza Internazionale. 2013;3:43-51.
- Queral-Godoy E, Valmaseda-Castellón E, Berini-Aytés L, Gay-Escoda C. Incidence and evolution of inferior alveolar nerve lesions following lower third molar extraction. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005;99(3):259-264.
- Renton T, McGurk M. Evaluation of factors predictive of lingual nerve injury in third molar surgery. Br J Oral Maxillofac Surg. 2001;39(6):423–428.
- Robert RC, Bacchetti P, Pogrel MA. Frequency of trigeminal nerve injuries following third molar removal. J Oral Maxillofac Surg. 2005;63(6):732-735.
- Rood JP, Shehab BA. The radiological prediction of inferior alveolar nerve injury during third molar surgery. Br J Oral Maxillofac Surg. 1990;28(1):20-25.
- Sedaghatfar M, August MA, Dodson TB. Panoramic radiographic findings as predictors of inferior alveolar nerve exposure following third molar extraction. J Oral Maxillofacial Surg. 2005;63(1):3-7.
- Sunderland S. A classification of peripheral nerve injuries producing loss of function. Brain. 1951;74(4):491-516.
- Jerjes W, Upile T, Shah P, Nhembe F, Gudka D, Kafas P, et al. Risk factors associated with injury to the inferior alveolar and lingual nerves following third molar surgery – revisited. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;109(3):335-345.
- Zuniga JR. Management of third molar-related nerve injuries: observe or treat? Alpha Omegan. 2009;102(2):79-84.

