Dr. Arun Garg illustrates how Flexo-Plate Plus was beneficial during rehabilitation of the atrophic anterior maxilla.
Dr. Arun K. Garg discusses a new and novel biomaterial
Loss of teeth in the anterior maxilla generally leads to severe resorption of the facial plate, resulting in osseous dimensions that will not accommodate implant placement. Resorption of the facial plate can also be an unexpected finding at the time of extraction when a tooth has undergone endodontic, periodontal, or structural changes. This condition is often complicated by the presence of natural dehiscences and fenestrations around healthy teeth that worsen when pathology arises.
The treatment methods most commonly employed for reconstruction of the deficient anterior maxilla follow:
- Onlay cortical bone blocks harvested intra- or extraorally and fixated with screws
- Particulated autogenous bone contained by a titanium mesh cage
- Ridge-split with interpositional bone grafting
While ample evidence of the efficacy and predictability of these methods can be found in the literature, the disadvantages associated with them are equally well documented. Cortical blocks require a separate donor site, leading to greater morbidity and patient discomfort during healing. Furthermore, resorption has been reported to occur during healing in 5% to 28% of cases.1 Similarly, the use of titanium mesh to contain particulate bone requires a second surgery (with added pain and morbidity) to remove the metal mesh and screws, making this option unattractive for many patients. Moreover, premature exposure of the mesh is a major complication of this technique.2 Because it requires a minimum ridge width to be successful, ridge splitting as a treatment option is unavailable to many patients. And when adequate initial ridge width is present, wound dehiscence and fracture of the facial plate may occur as the result of a bad split.3
This article describes an innovative method of restoring the atrophic anterior maxilla using a novel biomaterial that is configured to avoid the disadvantages associated with current treatment options. In this method, sheets of partially decalcified allogeneic bone fabricated into flexible bone plates (Flexo-Plate Plus, OsteoLife) are trimmed to conform to the osseous dimensions of the facial bone plate. Flexo-Plate Plus is a slightly malleable, 0.75 mm to 1.0 mm thick, partially decalcified allograft that comes with holes predrilled on the left and right aspects to accommodate fixation screws. Particulate bone graft material is placed over the defect, and the flexible bone plate is screw-fixated over it to stabilize the graft. Its matrix is gradually resorbed by the body and becomes part of the host bone, eliminating the need for surgical removal.
The biocompatible Flexo-Plate Plus is pliable enough to adapt to the contours of a skeletal defect yet strong enough to serve as a scaffold for graft containment without the risk of displacement. Its advantage over the use of cortical blocks is that the resulting bone has a medullary quality with active bone progenitor cells that come in contact with the implant surface. Ideally, implants should be placed into medullary bone, which is dynamic and active. Cortical bone is denser, but it contains few if any osteoblasts and other bone-maintaining cells. After healing, the bone in contact with the implant may appear dense, but it has less capacity to respond to changes related to the function of the implant. Compared with titanium mesh, the Flexo-Plate Plus has a very low risk of exposure because the body does not identify it as foreign. Moreover, it does not require surgical removal, as it converts to host bone during healing.
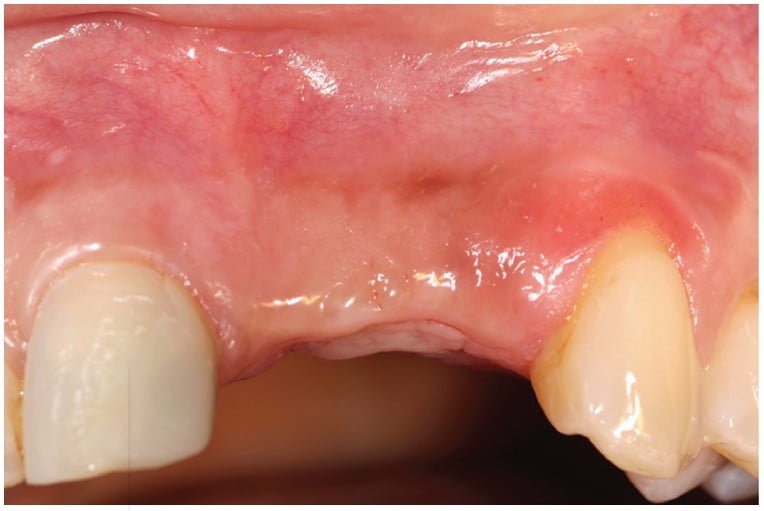
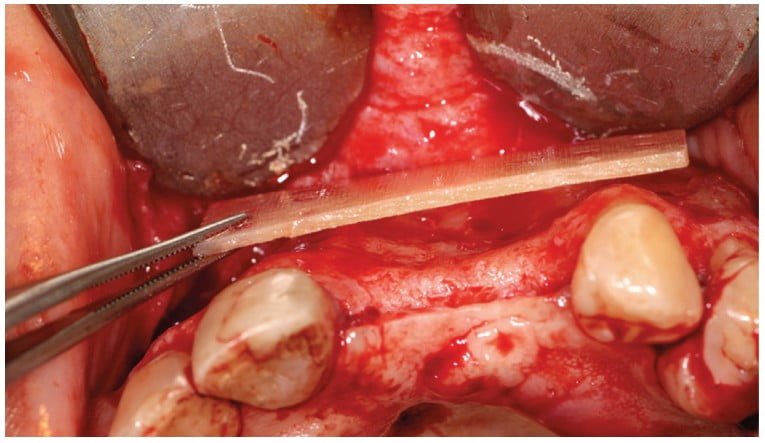
Figures 1 to 4 present the pre- and posttreatment images of a 52-year-old patient who presented with an atrophic anterior maxilla following extraction of the left central and lateral incisors 8 years earlier. Two-stage treatment involved the use of a Flexo-Plate Plus to cover particulate bone shavings mixed with platelet-rich plasma (PRP) to rebuild the deficient ridge, followed by a 4-month healing period prior to implant placement. As these images show, adequate thickness of the facial bone was obtained to house and provide long-term stability for two implants to replace the missing teeth.

After reading about Flexo-Plate Plus, read Dr. Garg’s article describing computer-guided surgery to restore function and esthetics with the FAIR Protocol at: https://implantpracticeus.com/computer-guided-surgery-to-restore-function-and-esthetics-in-partially-and-fully-edentulous-patients-the-fair-protocol/.
- Lee HG, Kim YD. Volumetric stability of autogenous bone graft with mandibular body bone: Cone-beam computed tomography and three-dimensional reconstruction analysis. J Korean Assoc Oral Maxillofac Surg.2015;41:232-239.
- Lim HC, Lee JS, Choi SH, Jung UW. The effect of overlaying titanium mesh with collagen membrane for ridge preservation. J Periodontal Implant Sci. 2015;45:128-135.
- Gurler G, Delilbasi C, Garip H, Tufekcioglu S. Comparison of alveolar ridge splitting and autogenous onlay bone grafting to enable implant placement in patients with atrophic jaw bones. Saudi Med J.2017;38(12):1207-1212.
Stay Relevant With Implant Practice US
Join our email list for CE courses and webinars, articles and mores

