Dr. Charles D. Schlesinger came to the aid of this patient, reversing the implant failure with a technique that combined mechanical, laser, and chemical procedures. Read about this implant success story here.

Dr. Charles D. Schlesinger discusses a technique to increase implant predictability
Implant treatment is a very predictable clinical procedure with a 10-year success rate reported to be 94.6%1; but sometimes unexpected sequelae can interfere with this high success rate.
The possible causes of failure can run the gamut from iatrogenic damage by the clinician who placed the implant, failure to properly manage existing bone loss, management of soft tissue, and the inability to achieve sufficient primary stability.
Immediate implantation at the time of extraction has many advantages. One of the biggest advantages is the drastic decrease in overall treatment time for the patient. In today’s world of instant gratification, an average decrease in treatment time from 7 to 8 months in traditional extract/graft/wait/place/wait protocol to a much more palatable 3 to 4 months is a true practice builder.2
Immediate implant placement has been shown to be as successful as delayed placement. The key to being able to provide either one of these treatment options is having the ability to achieve outstanding primary stability of the implant upon placement.3 This primary stability is necessary for successful osseointegration of the dental implant. Without it, micromovement of as little as 100 microns can result in soft tissue encapsulation and failure.
When done correctly, immediate implantation is as successful as delayed placements.
Mijiritsky, et al., investigated the long-term survival of single-tooth implants immediately placed in fresh extraction sites with a 6-year follow-up. In this study, 24 implants were placed in fresh extraction sites in 16 patients. The results demonstrated an overall implant survival rate of 95.8%. The study concluded that successful osseointegration can be accomplished with IL implants in fresh extraction sites. The peri-implant conditions were also stable till the 6th year of follow-up.4

Case study
A 78-year-old male patient presented to the office with a failed tooth No. 30, which was unrestorable due to the periodontal bone loss associated with it. A treatment plan discussion with the patient covered options such as extraction with grafting and eventually placing an implant 3 to 4 months later versus extraction with immediate placement. The patient chose to have the implant placed at the same time as the tooth removal, and since the success rate of immediately placed implants is very high, this decision was a prudent one.

After thorough review of the medical history, the patient’s only pertinent medical issue was Type 2 diabetes, which was under control. Implant survival in diabetics is 96.4%. Patients with poorly controlled diabetes have lower stability at the first 2 to 6 weeks. In the following weeks, stability reaches the baseline again, but reaching baseline takes 2 times the duration it needs in the healthy treatment group. Looking at the implant stability 1 year after implantation, there is no difference between the groups.5

After profound anesthesia with an inferior alveolar block and a long buccal infiltrate using 2% lidocaine with 1:100K epinephrine, a periotome was used to first sever the soft tissue interface around the tooth. A spade proximator, followed by 301 and 34 elevators, was used to luxate the tooth. Finally, a 151 forceps was used to facilitate the removal the tooth. The resulting socket was thoroughly debrided using a small curette and aggressive round diamond burs (Impladent Ltd.) on a surgical handpiece with irrigation. The buccal plate at the crest was thin, but intact.
Following recommended protocol, a 7 mm x 8 mm Hahn™ Tapered Implant (Glidewell) was placed with 45N/cm of torque and an ISQ values of 63/63. The resulting gap was grafted with allograft cortical/cancellous particulate (Newport Medical) and covered with a resorbable 3 to 4 month collagen membrane (Newport Medical) and sutured with 4.0 PGA suture.

Unfortunately, when the patient returned at his 2.5-week postoperative check, he had torn loose a few of his sutures (while eating caramel corn and getting it stuck in the sutures), and the underlying membrane now was exposed. The tissue had already gone through wound contracture, so re-suturing was not an option at that point. A 0.12% chlorhexidine rinse (Henry Schein®) was added at this time to the patient’s daily regimen, and the patient was scheduled for a follow-up in 1 month to evaluate healing.
Implant treatment is a very predictable clinical procedure with a 10-year success rate reported to be 94.6%
Follow-up
Unfortunately, when the patient returned, we were faced with bone loss and subsequent soft tissue loss which exposed the micro-threads of the implant to the oral environment (Figure 1). The collagen membrane was dissolved due to the harsh environment of the oral cavity. Once this occurs, biofilm contaminated the roughened implant surface, and then bone or soft tissue loss likely continued. A radiograph showed the current condition of the implant (Figure 2) with evidence of bone loss. Treatment options were discussed with the patient; either remove the implant or try and save it. He decided to try and save the implant.

After local anesthesia was attained with an infiltrate of 4% Septocaine® w/1:100K epi (Septodont), the soft tissue was first reflected to expose the top of the implant (Figure 3) and then crestal bone beyond the defect. The resulting defect exposed the micro-threads along with 2 mm of macro-threads (Figure 4). All granulation tissue was removed from the site and the implant body with mechanical debridement using curettes and a small wire brush.
After flushing with copious amounts of saline, a Sol® diode laser (DenMat) (Figure 5) was set to the perio setting, which is 1.5W. The implant surface was decontaminated with short pulses (Figure 6) until the surface appeared clean of any debris (Figure 7). It is important to make sure that you do not heat up the implant while doing this. Finally, the surface was wiped down with EDTA on a cotton pledget and finally rinsed with sterile saline.
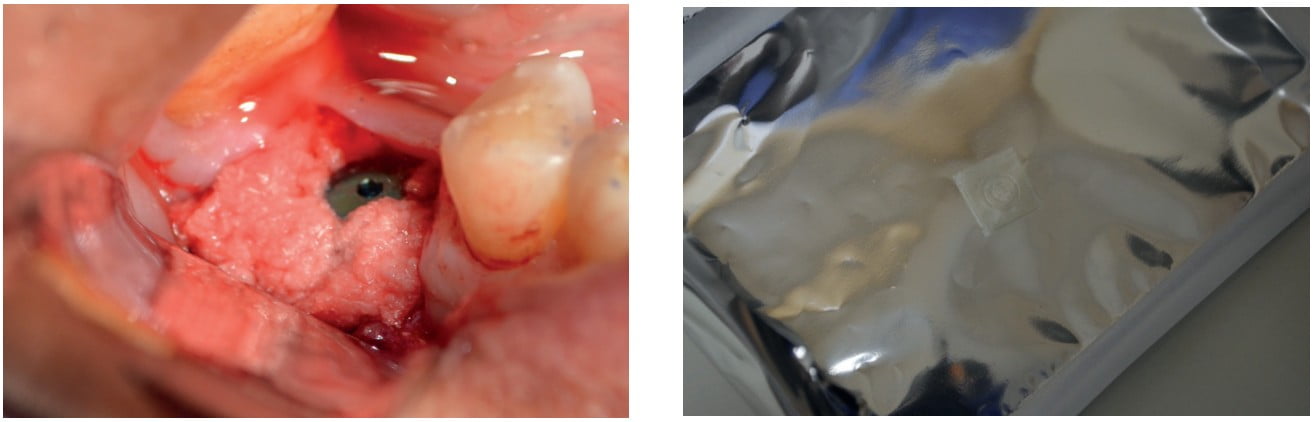
The surrounding bone was decorticated with a No. 2 carbide round bur to induce bleeding and stimulate new bone growth. The site was grafted with OsteoGen® plug alloplastic material (Figure 8) and then covered with a BioXclude® amnion-chorion membrane (Snoasis). The BioXclude membrane provides growth hormones and has been shown to help with accelerating the soft tissue wound closure (Figure 9).
The choice to use an alloplastic material instead of allograft for this revision surgery was just a personal choice. The OsteoGen material does not migrate like particulate, and this is important since the BioXclude is not robust enough to effectively contain large amounts of graft material. Literature has shown that both categories of grafting material are equally effective in regenerating bone in both quantity and quality.6
Finally, the soft tissue was closed with 4.0 PTFE suture (Figure 10) after placing a flat healing screw. The platform of the implant provided a tenting aspect to the site to alleviate any downward pressure on the graft by the healing soft tissue. Post-operative instructions included rinsing with 0.12% chlorhexidine in addition to normal oral hygiene.
The site was allowed to heal for 3 weeks before suture removal and then an additional 3.5 months before placement of a healing abutment. Keratinized tissue was laterally moved at this time to facilitate a ring of keratinized tissue around the healing abutment. The concave design of the Hahn healing abutments allows the tissue to be sutured in position and hold the level nicely. Once the soft tissue healed (Figure 11), we moved to the impression phase. VPS impressions were taken followed by placement of a final BruxZir® Esthetic screw-retained restoration (Glidewell Lab) (Figure 12).
At the 1.5 year follow-up, the hard and soft tissues were healthy (Figure 13), and the patient had reported no issues in the ensuing time period.
Conclusion
The keys to be successful in this kind of treatment are to start with an implant with excellent primary stability, the ability to thoroughly decontaminate the implant surface, providing adequate blood supply for regeneration, and finally assuring that soft tissue pressure will not impede bone growth.
Primary stability is paramount to the success of any implant treatment. The initial ISQ of 63/63 was excellent, and follow-up ISQ readings were 68/70 at the repair surgery and 77/77 at the time of restoration.
In order to provide an adequate framework for new bone growth onto the implant body, the surface of the implant must be brought as close to the cleanliness of a new sterile implant as possible. By the nature of implant surfaces, which are extremely porous due to the osteoconductive surface treatments provided by manufacturers, it is difficult to completely remove all presence of organic substances from the microtopography. The combination of mechanical, laser, and chemical means provides a way to clean the surface to a point that new bone growth will occur.
Although removing the implant at the early stage of healing would not have been a bad option and likely would have carried with it better overall chance of success, the ability to do large repairs like this can instill the confidence needed to routinely take on small grafting needs when healing does not proceed as planned.
From reversing implant failure to immediate loading implants, Dr. Schlesinger provides Implant Practice US readers with the insights of his experience. Read “From edentulous space to walking out with a tooth: a 40-minute experience,” here: https://implantpracticeus.com/from-edentulous-space-to-walking-out-with-a-tooth-a-40-minute-experience/
- Moraschini V, Poubel LA, Ferreira VF, Barboza E. Evaluation of survival and success rates of dental implants reported in longitudinal studies with a follow-up period of at least 10 years: a systematic review. Int J Oral Maxillofac Surg. 2015;44(3):377-388.
- Schlesinger C. Immediate implant Placement: cutting treatment time in half. Implant Practice US. 2015;8(5):20-24.
- Schlesinger C. Immediate Placement of Dental Implants: A Safe, A Predictable Treatment Option. J Dent Sci. 2016;4(3):146-152.
- Mijiritsky E , Mardinger O, Mazor Z, Chaushu G.. Immediate provisionalization of single-tooth implants in fresh-extraction sites at the maxillary esthetic zone: up to 6 years of follow-up. Implant Dent. 2009;18(4):326-333.
- Naujokat H, Kunzendorf B, Wiltfang J. Dental implants and diabetes mellitus—a systematic review. Int J Implant Dent. 2016; 2(1):5.
- Sezavar M, Bohlouli B, Hosein M, et al. Socket Preservation: Allograft vs. Alloplast. J Cytol Hist. 2015;S3(1).
Stay Relevant With Implant Practice US
Join our email list for CE courses and webinars, articles and mores

